The American Parkinson Disease Association (APDA) held a webinar in December focused on the role and effectiveness of modern medications in Parkinson’s disease (PD) progression, and described two drug therapy approaches. The speaker, movement disorder specialist Dr. Drew Falconer, detailed how contemporary (modern) drug therapy is far superior and preferred in comparison to the classic paradigm for drug therapy. Dr. Falconer noted that today (modern drug therapy) we have 23 medications to treat PD and 12 of them did not exist five years ago. Additionally, Dr. Falconer explained the importance of diagnosing PD correctly as many times PD-like symptoms happen to be parkinsonism but not Parkinson’s disease.
Here is an interesting excerpt from Dr. Falconer:
“When PD becomes overwhelming, take a deep breath and think about it just as a chemical problem. And if it’s just a chemical problem, we need to treat ourselves in a better way so our lives are smoother on a day to day basis.”
This APDA webinar was recorded, and is accessible on YouTube.
For more resources on medication, please see this Stanford Parkinson’s Community Outreach webpage:
Medications for Parkinson’s Disease
See my notes below for the session.
Regards,
Sheela Sakariya
“Until there’s a cure: living your best life with Parkinson’s disease” – Webinar notes
Webinar Host: American Parkinson Disease Association (APDA)
Webinar Date: December 17, 2021
Speaker: Drew Falconer, MD, movement disorders specialist, Virginia Commonwealth University
Summary by: Sheela Sakariya, Stanford Parkinson’s Community Outreach
Parkinson’s disease in 2021
There are many new frontiers in research and care for Parkinson’s disease (PD) that did not exist 15-20 years ago. We are making progress in finding more medications to help symptoms for PD. Today, we have 23 medications to treat PD and 12 of them did not exist five years ago.
Have the courage to talk to someone about how your day is going and how your medicine is letting you down or helping you. Essentially we want you to talk about why you can’t do what you want to do and keep advocating for yourself and the disease.
Parkinson’s disease statistics
PD is the second fastest growing neurological disease today. We are currently treating 1 million people in the US for PD. By 2030, it is estimated that we will be treating 1.2-1.5 million people with PD in the US. Among folks over the age of 60, 1 in 100 already have PD. We are diagnosing between 60,000-80,000 people every year with PD.
It’s important to educate yourself if you have been diagnosed and advocate for yourself – find others under similar circumstances and comfort yourself in knowing that you are not alone. There are many others in similar situations and looking for the same group camaraderie.
What is PD?
PD is not a structural problem – this is not a disease that comes from a tumor, mass or stroke. PD does not represent permanence of injury. For example, after a stroke, part of the brain is permanently damaged. The structure of the brain is not a problem in PD, but PD means there is a chemical deficiency in the brain. That chemical that the PD individual is lacking is dopamine! WIth dopamine deficiency, an individual is not getting enough dopamine which results in movement disorders. When there is too much dopamine, you see dyskinesia (excessive movements). Dyskinesia is a side effect of the medicine, not a symptom of PD.
When PD becomes overwhelming, take a deep breath and think about it just as a chemical problem. And if it’s just a chemical problem, we need to treat ourselves in a better way so our lives are smoother on a day to day basis.
PD is not an inherited disease and classically not something that runs in families. There can be several factors that cause PD including:
- Pesticides including Agent Orange
- Well water
- Heavy metal exposure
- Chemical exposure
- Head injury
Diagnosis of PD
It’s extremely important to diagnose PD correctly as there are still people who get misdiagnosed. Proper diagnosis is key to proper treatment! The most common way to diagnose PD is to note the individuals’ symptoms and history that they present to us. After that, we do a quick exam to check the symptoms. In most cases, we will give dopamine medications that will show you the benefits of the medications. Using the medications will make the PD symptoms better.
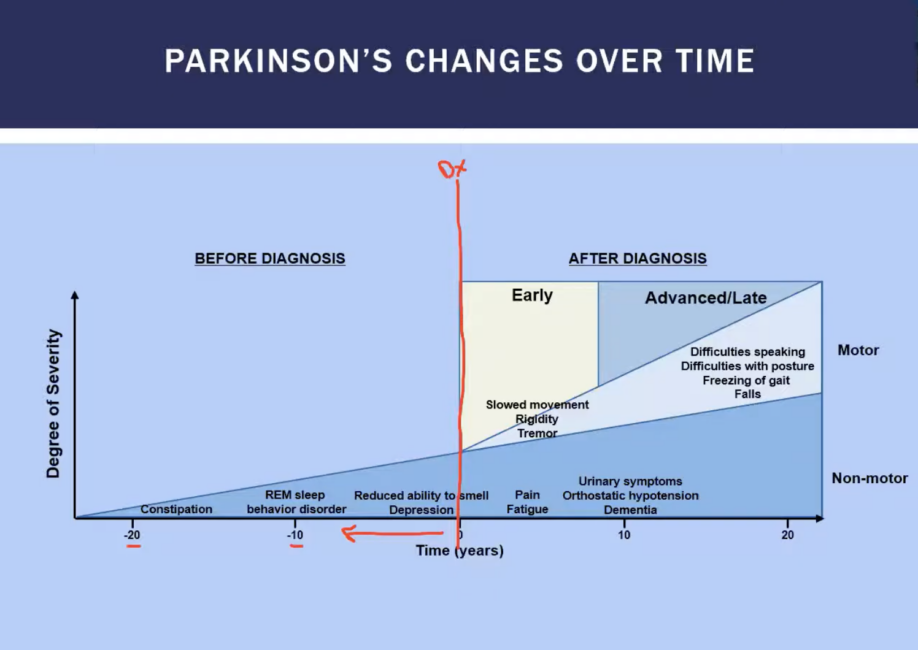
PD starts many years before diagnosis (perhaps 10-20 years before diagnosis). It takes the brain to be dopamine deficient by about 60% for the motor symptoms to start showing such as tremor, shaking, trouble walking. When the brain is about 30% down, the triad of symptoms include constipation, REM behavior-sleep disorder, and reduced sense of smell. So, the progression for PD is slow – 20 years to see initial symptoms.
OFF Time
Know what you feel! Part of your day is trying to maintain the amount of dopamine in your brain and part of your day will be when the medicine lets you down and the symptoms are coming out. That latter part of the day in PD is called the “OFF” time. Talk to your doctor about the OFF time and if we can fix the OFF time, then we can fix PD.
OFF time can happen anytime and it’s best to keep track of it. Types of OFF time include:
- First AM off
- End of dose
- Suboptimal on
- Sudden off
- Dose failure
- Exercise-induced
- Food-induced
70% reported 2+ OFF episodes a day
65% reported 2 or more hours a day
50% moderate/severe, affected daily activities
Mimickers of PD
With PD, the healthcare professional will give you medication and the symptoms get better. With Parkinson-isms, a person may suffer from the same symptoms as PD but there is limited medication response. Some of the Parkinson-isms include
- Vascular Parkinson’s
- Medication induced Parkinson’s
- Parkinson’s plus syndromes
- Multisystem atrophy
- Progressive supranuclear palsy
- Corticobasal degeneration
DIfferent approaches to therapy: Contemporary/modern approach is preferred
Classic treatment paradigm
- Pulsatile and frequent
- Higher and higher doses
- Leads to fluctuations
- Early side effects
- Treatment horizon
Contemporary treatment paradigm
- 23 different medications that stabilize dopamine
- Predictable and long acting
- Low doses, multiple targets
- “Rational polypharmacy” – use different medications to target different symptoms
- Employ technology earlier
- Smoother
- Reduced side effects
Medication categories for PD
New dopamine (levodopa) approach:
Rytary (carbidopa/levodopa)
- Updated formulation to deliver carbidopa-levodopa
- Can last from 5-8 hours compared to 2-3 hours for sinemet
- 1-2 hours less off time
- 2 hours more on time without dyskinesia
Non-dopamine approach:
Indirect pathway – activation reduces motor activity
- Direct pathway increases activity (dopamine, etc.)
- Indirect pathway inhibits motor activity (adenosine, GABA)
Adenosine A2a receptor antagonist
- Double neg locks the block
- Improves off times, releasing the “brake” on the system
Maximize your levodopa:
Ongentys (opicapone)
- 1x daily inhibitor of COMT enzyme
- Boosts levodopa for 24 hours
- Blocks breakdown of levodopa in the periphery, making more available to the brain
- In use in europe since 2016
- Once daily at bedtime away from food
Dyskinesia and OFF episodes
Gocovri (amantadine ER)
- 1st daily amantadine ER at bedtime
- First “FDA approved” therapy for dyskinesia AND off periods
- Used to reduce dyskinesia (37% reduction or elimination)
- Reduced OFF time by 45% during the day
Rescue option 1
Apokyn (apomorphine injection)
- Rapid onset dopamine agonist via injection
- For different types of OFF episodes:
- Rapid off, wearing off
- Dose failure/unexpected off
- Delayed on
- First AM symptoms or exercise intolerance
- Achieve ON within 10-20 minutes
Rescue option 2
Inbrija (levodopa inhalation powder)
- Rapid onset levodopa through inhaler
- For different types of OFF episodes:
- Rapid off, wearing off
- Dose failure/unexpected off
- Delayed on
- First AM symptoms or exercise intolerance
- Achieve ON within 10 minutes, can take upto 5x daily
Rescue option 3
Kynmobi (apomorphine sublingual film)
- Sublingual dissolving film for “off” episodes
- Improvement begins after 15 minutes
- For different types of OFF episodes:
- Rapid off, wearing off
- Dose failure/unexpected off
- Delayed on
- First AM symptoms or exercise intolerance
- Can take upto 5x daily
Orthostatic hypotension (OH)
Northera (droxidopa)
- OH is common symptom of PD
- Can be worsened by dopamine supplementation
- Prodrug (precursor of a drug) for Norepinephrine, crosses BBB
Future medications and technologies lead us to hope for better treatment of PD
- Longer acting levodopa formulation (10 hours or greater)
- New inhibitors
- Pump-based and subcutaneous formulations
- Improved technology
- Targeted protein therapy
- Cure