
Parkinson’s disease (PD), which affects movement, and Alzheimer’s disease (AD), which affects memory, seem like distinct conditions. Research reveals these brain disorders share biological patterns. In January 2026, The Michael J. Fox Foundation hosted a wide-ranging panel discussion exploring how Parkinson’s, Alzheimer’s, and Lewy body dementia overlap, from symptoms to shared protein changes in the brain.
The panel included Dr. Melissa Armstrong, a movement disorder specialist who directs Lewy body dementia research at the University of Florida, Dr. Tom Tropea, chief medical officer at the Institute for Neurodegenerative Disorders, and Fred Goldstein, who has cared for his father with Lewy body dementia and his mother with Alzheimer’s. Katie Kopil, senior vice president and head of clinical research at The Michael J. Fox Foundation, moderated.
The panelists also addressed environmental factors that add to disease risk, the value of exercise for both physical and cognitive symptoms, and emerging biomarker tests that could lead to precision treatments. Fred Goldstein shared his family’s experience navigating two different neurodegenerative diagnoses and his decision to participate in research, including genetic testing that revealed his own increased risk for Parkinson’s.
Watch the full webinar: register on the MJFF website to watch on demand
Webinar slides (PDF): Exploring the Link Between Parkinson’s and Alzheimer’s
Related resources from the Stanford Parkinson’s website:
Resources mentioned in the webinar:
- Parkinson’s Progression Markers Initiative (PPMI) – Landmark research study developing biomarkers and recruiting volunteers with and without Parkinson’s to advance precision medicine
- ClinicalTrials.gov – Database of clinical studies for Parkinson’s, Alzheimer’s, and other conditions
The panel featured a conversation among panelists with audience questions addressed throughout. Now, on to my detailed notes. – Kevin
Exploring the Link Between Parkinson’s and Alzheimer’s
Panelists

- Katie Kopil: Senior Vice President and Head of Clinical Research,
The Michael J. Fox Foundation (moderator)

- Dr. Melissa Armstrong: Director, University of Florida Health Gorian Clinical Research Headquarters for Lewy body dementia at the Norman Fixel Institute for Neurological Diseases; movement disorder specialist

- Dr. Thomas Tropea: Chief Medical Officer, Institute for Neurodegenerative Disorders; Adjunct Professor of Neurology, University of Pennsylvania Perelman School of Medicine; movement disorder specialist
{kind=link}

- Fred Goldstein: Founder and President, Accountable Health; host of Pop Health Week radio show; care partner to his father who lived with Lewy body dementia and his mother who lives with Alzheimer’s
Webinar Date: January 15, 2026
Host: The Michael J. Fox Foundation (MJFF)
Summary by: Kevin Boyd, Stanford Parkinson’s Community Outreach
A Person Can Have Both Disorders
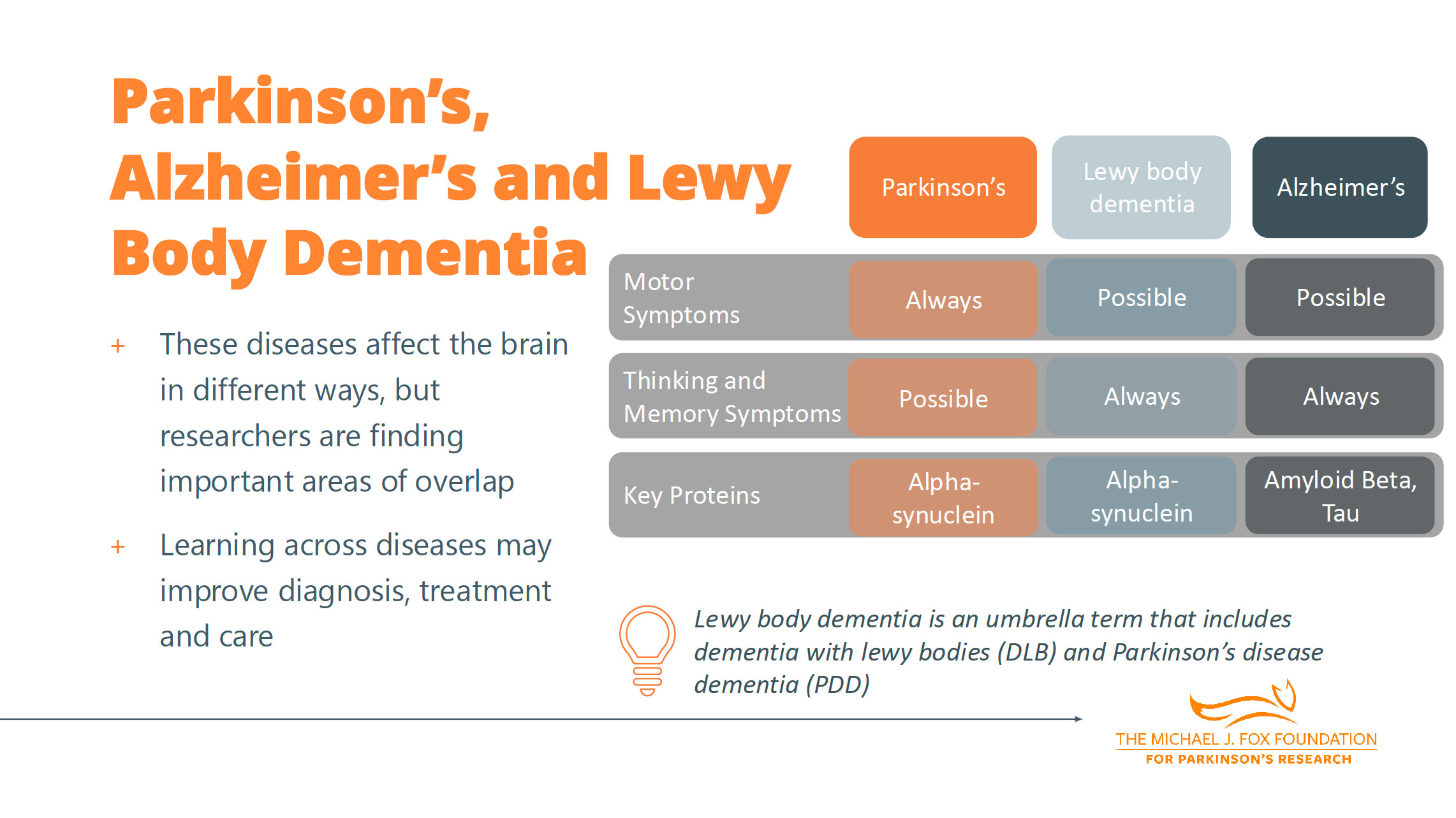
Dr. Tropea explained why these conditions are increasingly discussed together. The same person can develop the brain pathology or proteins that characterize Parkinson’s and the brain pathology or proteins that characterize Alzheimer’s.The clinical labels reflect which symptoms are most prominent, but the brain changes often overlap.
PD Statistics
Fred Goldstein provided context on how common PD has become. Roughly 1.1 to 1.2 million people in the United States are living with PD. A 2022 study found that nearly 90,000 people are diagnosed with PD every year in the United States, up considerably from about 60,000 just a few years earlier. PD is now the fastest-growing neurological disease in the world, with rates up about 50% from previous estimates. By 2050, researchers estimate about 25.2 million people globally will be living with PD.
A Family Journey
Goldstein shared his personal experience caring for family members with different neurodegenerative conditions. His father was diagnosed with dementia with Lewy bodies and, later, his mother was diagnosed with Alzheimer’s. The caregiving effort for the family has been significant. Goldstein says that caregivers need to think about where the individual is and what they’re able to do.
With his father’s dementia with Lewy bodies, cognitive symptoms came first and early. It was a massive change for both parents and the family. His father had to retire from his work while still physically able, although he didn’t want to, which made it difficult.
Each of the kids had different skill sets and began helping based on their expertise. As an example, his father loved to fish. Goldstein would take him fishing, putting his father in a chair at the front of a boat wearing a life vest.
Hallucinations can be difficult. At a theater, his dad would suddenly say, “Hey, there are four people over there. What are they doing?”
Environmental Exposure
From his population health perspective, Goldstein noted that as we understand environmental risks better, people may need to change what they’re doing or what they’re getting exposed to. Back in the day it was, “Hey, my lawn’s got to look like XYZ and I’m going to put these chemicals on it.” Those are the kinds of associations he’s begun to recognize and hear others talking about as well. It’s important to talk to individuals who really know and understand it to get a better sense of what the risk means. Environmental exposure adds to potential risk. There are things we can do to try to minimize those add-on risks, whether it’s sleep, eating habits, or exposure to toxins.
Genetic Testing and Research Participation
Goldstein made the decision to do genetic testing when he saw a Facebook post from MJFF that said people at risk for Parkinson’s should be tested. His father had passed away at that point, and Goldstein wanted to help with research and know his own risk. In his genetic screening, a Parkinson’s risk variant showed up. This knowledge has helped him think through what his future might be like. His participation has created data that is helping the field advance and allowed him to learn things about his own health.
As a result of Goldstein’s genetic test, he decided to enroll in a study. Participating has been one of the great joys of his life, being able to say he’s doing something to potentially help himself down the road, but certainly others. It’s been a fantastic experience. The tests at the research site can be tough sometimes, but they work through that. As someone in the field of population health, he notes that data is the river that flows through population health, and what they’re trying to do is create more data. If people can participate or are interested, they should. It’s making a difference.
Understanding Diagnosis and Disease Biology
Diagnosis is Challenging
Dr. Armstrong explained what makes these conditions difficult to identify early. Symptoms start gradually rather than suddenly, making them harder to recognize. The symptoms themselves can be confusing to connect. People can have constipation as an early symptom without thinking it could be related to Parkinson’s.
Clinical Diagnoses Can Change Over Time
Dr. Tropea addressed why someone’s diagnosis might evolve. The symptoms that first bring someone to see a physician or neurologist may be just the first symptoms they experience. Maybe it’s tightness or rigidity in a limb, or perhaps memory changes or personality changes.
These disorders take time to manifest and take time to understand what is going on. A physician on a first visit might have a suspicion but can’t confirm the diagnosis because the person doesn’t yet meet the criteria. This happens frequently in clinical practice.
Part of the diagnostic challenge stems from limited tools. Great diagnostic tools outside of the clinical exam don’t exist yet. While some imaging techniques and new research tools are emerging, diagnosis still relies heavily on clinical observation and tracking how symptoms develop over time.
Understanding Lewy Body Dementia
Dr. Armstrong helped clarify the terminology around Lewy body dementia, acknowledging that the vocabulary is messy. The term Lewy body dementia actually includes two different diagnoses.
People receive the diagnosis Dementia with Lewy Bodies when memory and thinking problems are present right up front. They may have hallucinations and some Parkinson’s movement problems, but the main problem at the beginning is memory and thinking.
The diagnosis of Parkinson’s Disease Dementia is given to people who have a diagnosis of Parkinson’s based on their physical symptoms at the beginning, but then over the course of their disease they develop memory and thinking problems.
The term “Lewy body dementia” includes people with memory problems first (dementia with Lewy bodies) and people with Parkinson’s who develop memory and thinking problems later (Parkinson’s disease dementia).
The Overlaps and Differences in Symptoms
Dr. Tropea addressed the symptom overlap across these conditions. While Parkinson’s is known for motor symptoms like tremor and walking challenges, and Alzheimer’s for memory issues, the reality is more nuanced.
In Lewy body dementia (both Parkinson’s disease dementia and dementia with Lewy bodies), changes in thinking and memory differ somewhat from Alzheimer’s. People with Lewy body dementia have less pure memory loss (inability to recall things) and more hallucinations, difficulties with navigating space, and trouble ordering tasks.
In Alzheimer’s, movement changes can also occur. Sometimes there are overlapping symptoms, and a diagnosis is based on the primary syndrome, but people can experience many other symptoms across these conditions.
With all of these conditions, symptoms like lethargy, depression, anxiety, and constipation are very common. We don’t typically describe these as the primary symptoms of one disorder, but they can occur across all of them. When looking at data about what bothers people most, it’s often these other symptoms that people report.
Movement problems and memory are what bring someone to the doctor, but depression can be the biggest challenge, or daytime sleepiness, or lack of motivation.
Understanding Multiple Pathologies in the Brain
Dr. Armstrong explained that having both Parkinson’s-related changes and Alzheimer’s-related changes in the brain simultaneously is actually quite common, particularly as people age.
The clinical diagnosis typically reflects whichever set of symptoms is most prominent at any given time. If movement symptoms dominate, the diagnosis might be Parkinson’s disease. If memory and cognitive changes are more severe, it might be diagnosed as Alzheimer’s or Lewy body dementia.
Over half the people with dementia with Lewy bodies have Alzheimer’s changes in the brain. This biological complexity is one reason why developing effective treatments has been so challenging.Understanding Diagnosis and Disease Biology
Diagnosis is Challenging
Dr. Armstrong explained what makes these conditions difficult to identify early. Symptoms start gradually rather than suddenly, making them harder to recognize. The symptoms themselves can be confusing to connect. People can have constipation as an early symptom without thinking it could be related to Parkinson’s.
Clinical Diagnoses Can Change Over Time
Dr. Tropea addressed why someone’s diagnosis might evolve. The symptoms that first bring someone to see a physician or neurologist may be just the first symptoms they experience. Maybe it’s tightness or rigidity in a limb, or perhaps memory changes or personality changes.
These disorders take time to manifest and take time to understand what is going on. A physician on a first visit might have a suspicion but can’t confirm the diagnosis because the person doesn’t yet meet the criteria. This happens frequently in clinical practice.
Part of the diagnostic challenge stems from limited tools. Great diagnostic tools outside of the clinical exam don’t exist yet. While some imaging techniques and new research tools are emerging, diagnosis still relies heavily on clinical observation and tracking how symptoms develop over time.
Understanding Lewy Body Dementia
Dr. Armstrong helped clarify the terminology around Lewy body dementia, acknowledging that the vocabulary is messy. The term Lewy body dementia actually includes two different diagnoses.
People receive the diagnosis dementia with Lewy bodies when memory and thinking problems are present right up front. They may have hallucinations and some Parkinson’s movement problems, but the main problem at the beginning is memory and thinking.
Parkinson’s disease dementia is given to people who have a diagnosis of Parkinson’s based on their physical symptoms at the beginning, but then over the course of their disease they develop memory and thinking problems.
Lewy body dementia includes people with the memory problem first (dementia with Lewy bodies) and people with Parkinson’s who develop memory and thinking problems later (Parkinson’s disease dementia), the second type of diagnosis.
The Overlaps and Differences in Symptoms
Dr. Tropea addressed the symptom overlap across these conditions. While Parkinson’s is known for motor symptoms like tremor and walking challenges, and Alzheimer’s for memory issues, the reality is more nuanced.
In Lewy body dementia (both Parkinson’s disease dementia and dementia with Lewy bodies), changes in thinking and memory differ somewhat from Alzheimer’s. People with Lewy body dementia have less pure memory loss (inability to recall things) and more hallucinations, difficulties with navigating space, and trouble ordering tasks.
In Alzheimer’s, movement changes can also occur. Sometimes there are overlapping symptoms, and a diagnosis is based on the primary syndrome, but people can experience many other symptoms across these conditions.
With all of these conditions, symptoms like lethargy, depression, anxiety, and constipation are very common. We don’t typically describe these as the primary symptoms of one disorder, but they can occur across all of them. When looking at data about what bothers people most, it’s often these other symptoms that people report. Movement problems and memory are what bring someone to the doctor, but depression can be the biggest challenge, or daytime sleepiness, or lack of motivation.
Understanding Multiple Pathologies in the Brain
Dr. Armstrong explained that having both Parkinson’s-related changes and Alzheimer’s-related changes in the brain simultaneously is actually quite common, particularly as people age.
The clinical diagnosis typically reflects whichever set of symptoms is most prominent at any given time. If movement symptoms dominate, the diagnosis might be Parkinson’s disease. If memory and cognitive changes are more severe, it might be diagnosed as Alzheimer’s or Lewy body dementia.
Over half the people with dementia with Lewy bodies have Alzheimer’s changes in the brain. This biological complexity is one reason why developing effective treatments has been so challenging.
What’s Happening in the Brain: Misfolded Proteins
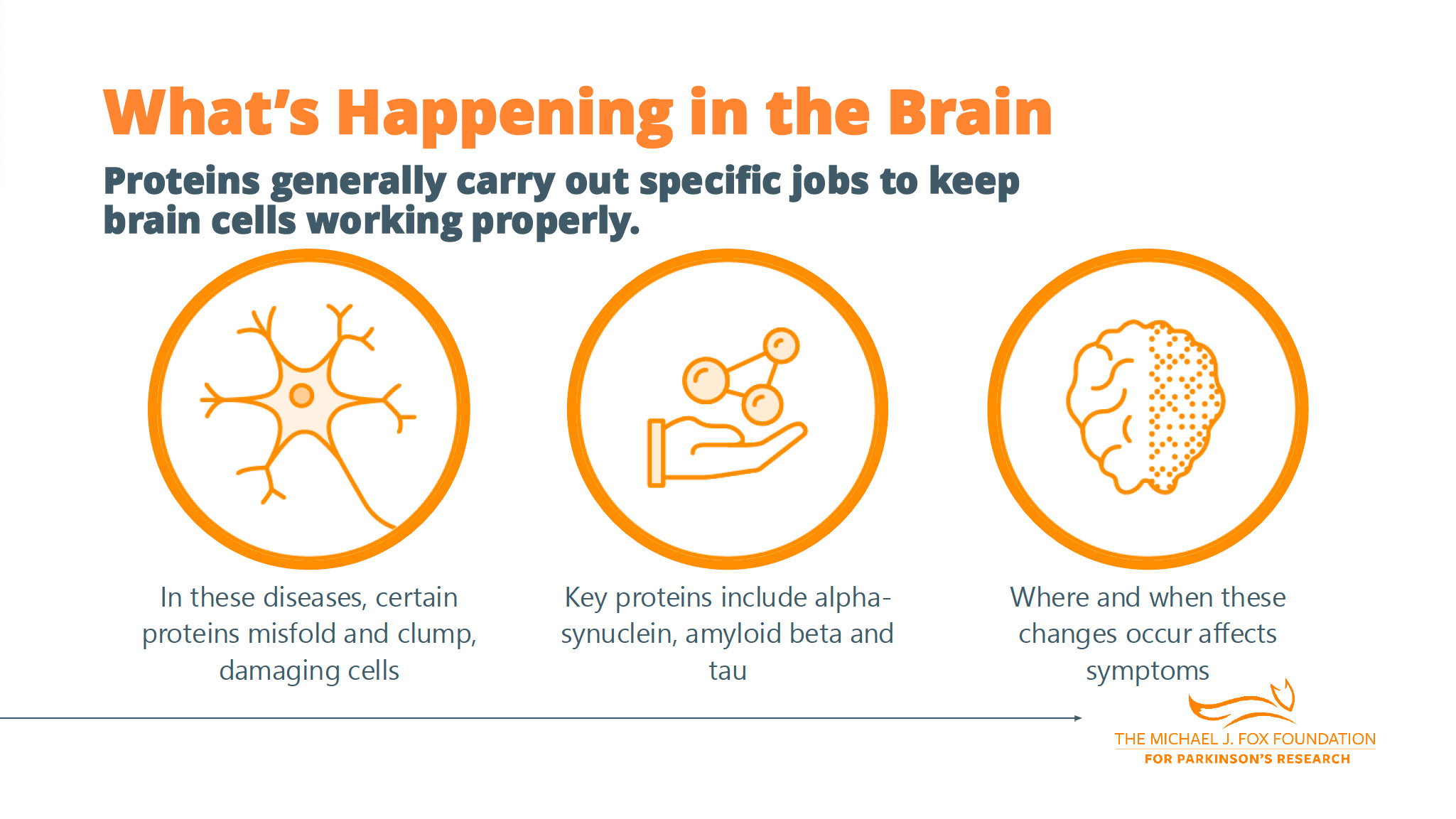
Dr. Tropea provided an overview of the underlying biology. Both Parkinson’s and Alzheimer’s are neurodegenerative disorders. One common theme is that proteins misfold for reasons researchers aren’t entirely sure of.
The proteins misfold into an orientation that either prevents the body from clearing them normally or induces clumping. When that happens, they accumulate in the brain.
Alpha-synuclein is the protein associated with Parkinson’s and dementia with Lewy bodies. Amyloid beta and tau are associated with Alzheimer’s. Even in people with Parkinson’s there can be some accumulation of amyloid and tau, and vice versa.
Where proteins deposit makes a difference. When diffuse alpha-synuclein is around the entire brain early, researchers think of that as dementia with Lewy bodies. When it occurs more focally, predominantly in the brainstem, researchers think that leads to Parkinson’s, at least early on. However, over time the proteins can migrate to different areas.
Diagnostic Tests: What’s Available and What’s Coming
Dr. Armstrong discussed the current state of diagnostic testing. Most of the time, diagnosis is still based on the doctor asking what symptoms someone has been having and doing a physical exam. This very core part of a doctor visit remains central.
But there are some emerging tests. For Parkinson’s and dementia with Lewy bodies, there’s a skin biopsy that some doctors will order now. Skin is taken from the back of the neck, near the knee, or near the ankle to look for signs of the alpha-synuclein protein in the skin.
For Alzheimer’s, Parkinson’s, and dementia with Lewy bodies, doctors can do a lumbar puncture with cerebrospinal fluid testing to look for the abnormal proteins.
In Alzheimer’s, there are some brain scans that can be used to help in diagnosis.
Environmental Exposures and Risk Factors
An attendee asked about environmental exposures linked to neurodegenerative disorders and whether those exposures are similar or different across Parkinson’s and Alzheimer’s.
Dr. Tropea explained how to think about risk. When discussing environmental exposures, he’s talking about the risk of developing Parkinson’s. He puts this into three risk categories: age, genetic makeup, and environmental exposure.
Age continues to increase as a risk factor over time. Genetic makeup stays relatively the same. Environmental exposure can be any number of things: certain toxins, eating habits, sleep habits. Lots of things go into environmental exposure that affect risk.
When most people discuss environmental risk, they’re referring to environmental toxins related to pesticides and proximity to certain areas that have high prevalence of certain toxins. Researchers are learning more about that.
The critical distinction: exposure to certain environmental risk factors adds to genetics and to age. In most scenarios, toxin exposure is not the absolute cause of symptoms. It adds to risk.
Research continues to identify which specific toxins pose the greatest risk.
The Value of Exercise
Dr. Armstrong addressed movement and exercise for people living with these conditions. “For people living with Parkinson’s in my clinic, every time I see them, we talk about how important it is to exercise and stay active,” she said.
The research is compelling. “There is lots of research showing that people with Parkinson’s who exercise do better and there are even ongoing research studies to look at whether exercise might even be able to slow the progression of Parkinson’s.”
But the benefits extend beyond just physical symptoms. Dr. Armstrong pointed to research outside of Parkinson’s showing that exercise benefits people living with mild cognitive impairment. “So, I think that one of the most important things people with Parkinson’s can be doing for both their physical health and their mental and cognitive health is making sure to have a regular exercise regimen and then staying physically and mentally active in other ways as well.”
What Type of Exercise Is Best?
When asked about the right type of exercise, Dr. Armstrong explained that different kinds of exercise have been studied in people with Parkinson’s, and different types might help in different ways. The most important thing is doing it consistently. She added that there’s probably no wrong time to exercise, though it doesn’t have to be every day.
She referenced a publication from the past year asking whether there could be too much exercise. “In my clinic, I encourage people to start slowly, ramp up and target three to four times a week.”
Dr. Tropea added his clinical perspective: “What I tell most of my patients in the office is that I’m not here to prescribe you a certain type of exercise. In fact, I think you’re much less likely to do it if it’s a prescription. It’s just whatever exercise you’re going to do every day. And that may be walking, it may be stretching, it may be yoga, it may be running a marathon, who knows? Whatever it is that you’re going to do, that’s the one that you should continue with.”
Katie Kopil reinforced this: “One of the things that I find helpful for myself and also for conversations with community members, the exercise that you’re going to stick with is the best one that you can do.”
Neuroinflammation as a Potential Treatment Target
Attendees asked about neuroinflammation as a driver across neurodegenerative disorders and what progress is happening to target it.
Dr. Tropea acknowledged they hadn’t been entirely comprehensive in their discussion. Although they were talking about Alzheimer’s and Parkinson’s changes in the brain, there are actually many other things that occur. They hadn’t discussed vascular changes or changes to blood vessels, and there are other proteins that can misfold and affect brain cells.
Inflammation is one of the pathways that can be affected in all neurodegenerative disorders. Is it a reactionary process where the alpha-synuclein may deposit and cause neuroinflammation, or is it that neuroinflammation precipitates or increases the risk of depositing alpha-synuclein into the cells? These are things researchers are learning about.
What we do know is that neuroinflammation is a potential target. There are drugs in development to target neuroinflammation.
Dr. Armstrong added that this is an area of current research, and we need to see where that research leads.
The Path Toward Precision Medicine
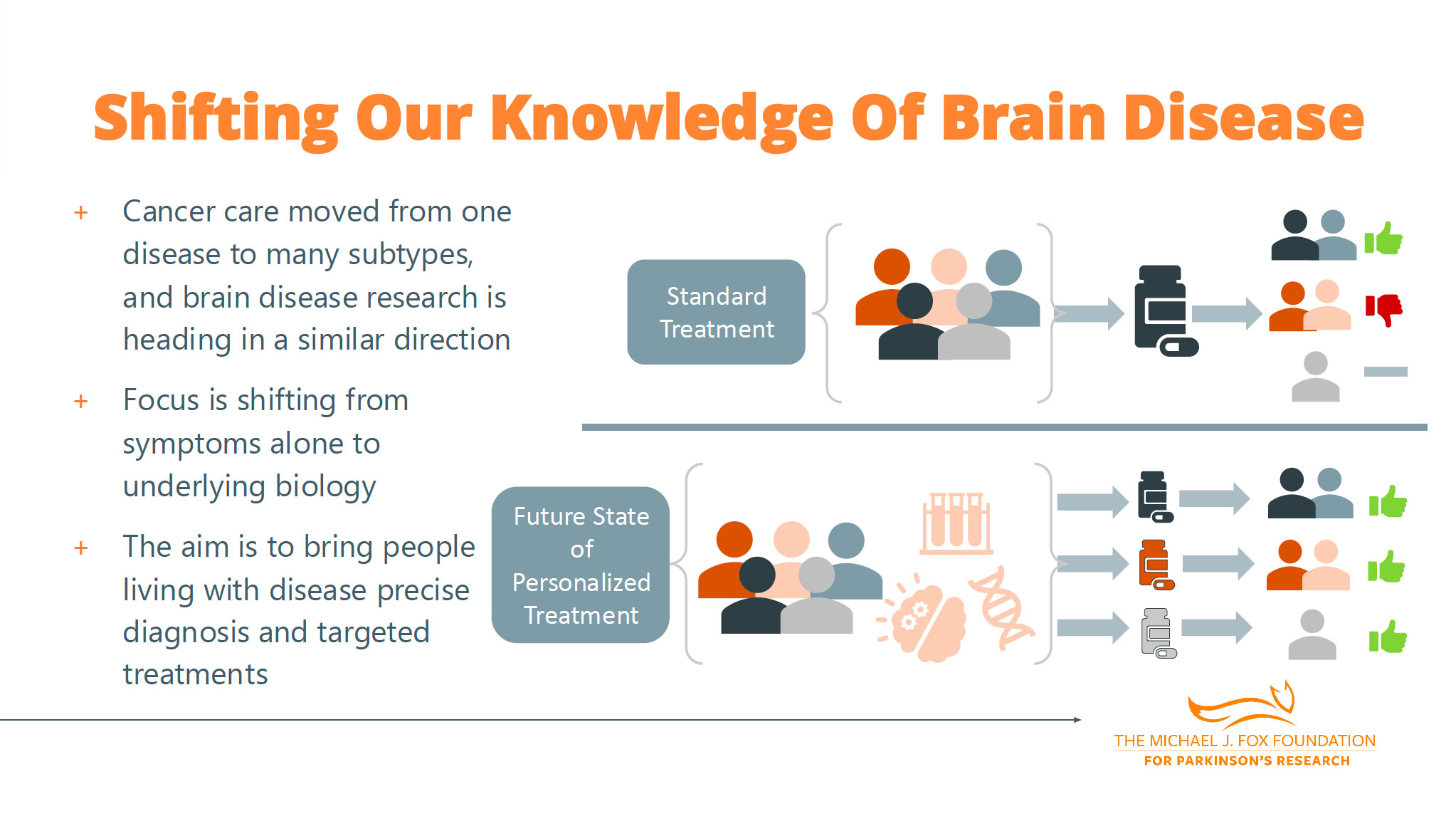
Dr. Tropea discussed the shift happening in the field, similar to what’s occurred in oncology. Cancer treatments used to be very broad, but now many cancers have targeted therapies and immunotherapies that target specific kinds of cancer. One of the most important transitions in oncology was the ability to detect abnormal cells.
In brain disorders, researchers can’t take out the bad parts, so they need to function in a system where they use biomarkers (blood tests, spinal fluid tests, or skin tests) to detect and predict what’s going on in the brain, along with imaging tests. “We’ve had some great breakthroughs in our ability to detect and measure the abnormal protein,” Dr. Tropea said.
One important development: we now know that people participating in Parkinson’s clinical trials actually didn’t even have alpha-synuclein in their brain. Researchers can now use tests to clarify who actually has the target protein.
The first step towards precision is using biomarkers, Dr. Tropea said.