
This webinar from February 2026 addressed frequently asked questions about physical therapy for people living with Parkinson’s disease (PD). Anyone with PD, their care partners, and family members seeking to understand how physical therapy can support mobility, independence, and quality of life will be interested in this topic.
Physical therapists Teresa Baker and Sara Crandall Zoeller from Boston University’s Center for Neurorehabilitation tackled the most common questions they hear: What does physical therapy actually involve? When should someone start? What’s the best exercise for Parkinson’s? The answers challenge some common assumptions, particularly the idea that physical therapy should wait until movement problems become obvious.
The presenters recommend people with Parkinson’s follow a model of care that treats physical therapy as an ongoing relationship rather than a one-time fix. This approach uses periodic check-ins to track changes over time and catch issues before they lead to falls or major disruptions. They also addressed practical concerns like insurance coverage, staying motivated between appointments, and whether someone who already exercises regularly still needs physical therapy.
Care partners play a critical role in supporting safe movement at home, and the webinar outlined specific ways they can help beyond just physical assistance. From understanding medication timing to making safety modifications at home, care partners have unique insights that physical therapists can build on.
The session wrapped up with audience questions covering home therapy versus outpatient care, managing pain, and maintaining exercise routines when fatigue becomes a barrier.
Watch the full webinar on the APDA YouTube channel:
Let’s Keep Moving With APDA: Frequently Asked Questions in Physical Therapy
Related resources from the Stanford Parkinson’s website:
Related resources from the American Parkinson Disease Association:
- Be Active & Beyond booklet (APDA)
- APDA Exercise Helpline (Boston University)
- APDA Community chapters (APDA)
Resource(s) mentioned in the webinar:
Now, on to my detailed notes. – Kevin
Frequently Asked Questions in Physical Therapy
Panelists

Dr. Teresa Baker: Physical therapist at Boston University’s Center for Neurorehabilitation

Dr. Sara Crandall Zoeller: Physical therapist at Boston University’s Center for Neurorehabilitation
Webinar Date: February 3, 2026
Host: American Parkinson’s Disease Association (APDA)
Summary by: Kevin Boyd, Stanford Parkinson’s Community Outreach
Understanding Physical Therapy for Parkinson’s
Physical therapy (PT) starts with an exam. Baker explained that therapists examine how someone walks, including speed, endurance, and quality of walking pattern. They assess balance from different angles, evaluate posture, and look at challenges in day-to-day life. The examination also covers strength, range of motion, and how PD symptoms like slowness and stiffness affect movement.
After gathering data and discussing needs with the patient, the physical therapist prescribes a personalized program. This includes exercise recommendations and often goes beyond just exercise. For people with PD, treatment frequently includes specific walking practice, balance training in the context of regular activities, and strategies for daily movements like getting up from a chair safely, rolling in bed, or getting in and out of a car.
When Should Someone Start Physical Therapy?
Baker emphasized: “Early and regularly.” Early means “as soon as possible upon diagnosis,” even before someone notices issues with movement or walking.
Physical therapy should also be considered whenever something changes, such as balance becoming more difficult or walking patterns shifting. Baker recommended treating PT as a regular practice, suggesting annual check-ins similar to neurologist visits, or dental cleanings.
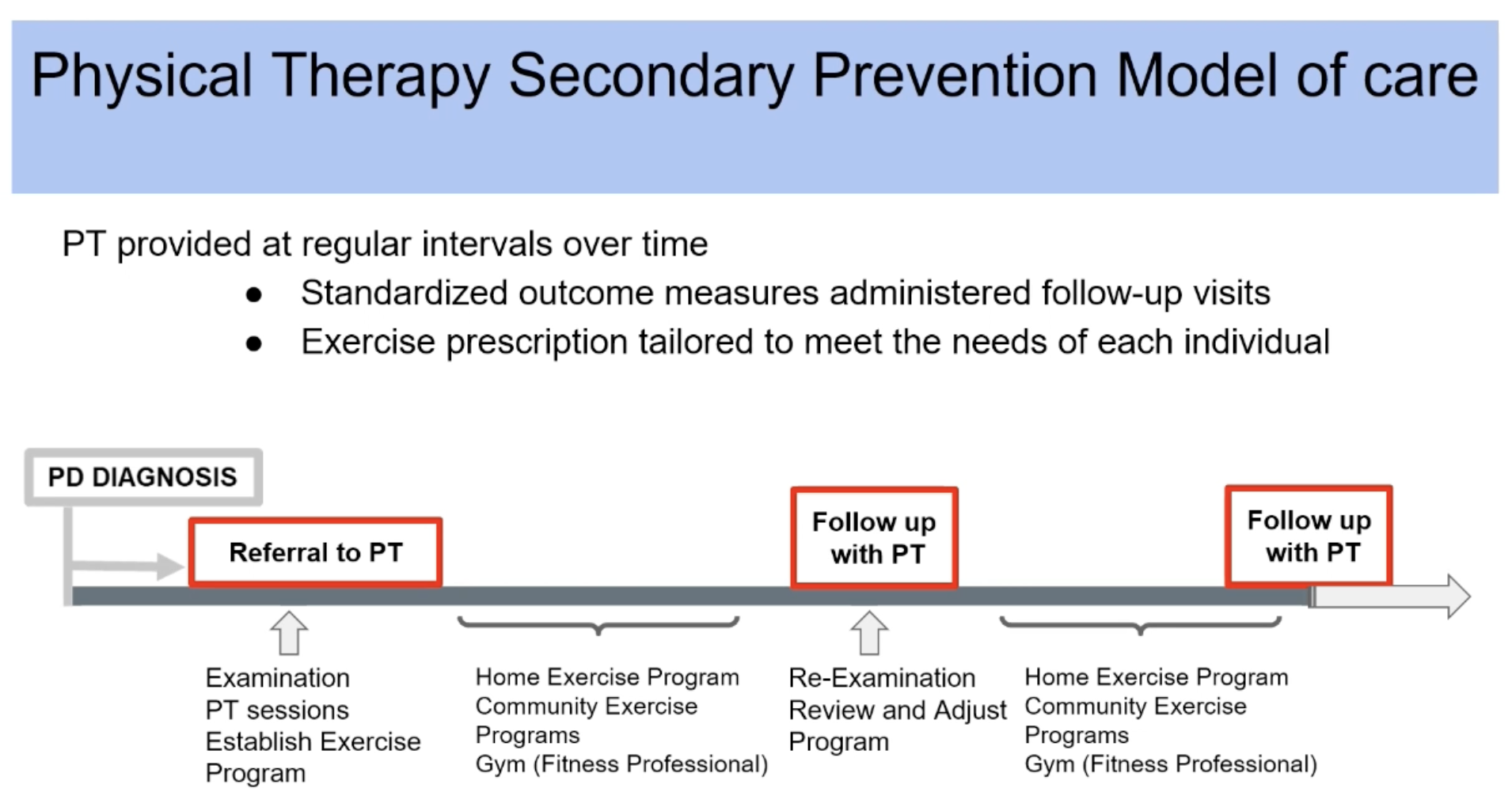
The Secondary Prevention Model Of Care
Boston University’s Center for Neurorehabilitation uses what they call a “secondary prevention model of care.” This approach uses PT to support health and mobility before limitations occur.
Under this model, someone diagnosed with PD receives an immediate referral to PT. The initial exam collects baseline data on movement. The therapist and patient work together over several visits to establish a realistic, effective program. When that episode of care ends, the person continues their exercise program independently, potentially joining community-based exercise classes or fitness center programs.
After roughly six months, the person returns for a new evaluation. The therapist reviews the program to determine if adjustments are needed or if everything remains on track. This might be just one or two tune-up sessions before ending that episode and continuing the exercise routine. This pattern repeats, allowing the therapist to track function over time and catch changes before they lead to falls or other disruptions.
What Is The Best Exercise For Parkinson’s?
Baker noted this is the most common question they receive. Her answer: there is no single best exercise for PD.
“The best exercise is the exercise that someone will do,” Baker said. The right program depends on how someone’s PD presents, what they enjoy, what’s safe and realistic, and what’s sustainable long-term.
Research supports multiple types of exercise as important for people with PD:
- Aerobic exercise: Moderate intensity aerobic activity seems effective for managing motor symptoms of PD. It increases heart rate, often causing sweating and heavier breathing. Examples include walking and bicycling.
- Strength training: Progressive overload training for major muscle groups can potentially slow or improve the slowness and stiffness associated with PD and help improve overall daily function.
- Flexibility training: This helps combat stiffness associated with PD and can be incorporated in various ways.
- Balance training: Critical for fall prevention, balance training should be personalized to individual needs and can include numerous activities.
The “Be Active” booklet, developed by Boston University’s center in conjunction with APDA, provides detailed recommendations on these exercise types with suggestions for how to work them into a program.
What Can Care Partners Do To Support Safe Movement At Home?
Care partners play a key role in safety at home through teamwork, coordination, and communication. Baker noted that care partners often know the person with PD best, understand the home routine, and know what works in the home.
Some care partners coordinate medication, giving them unique insight into how medication affects the person with PD throughout the day. They can recognize when medication works well and when the person experiences off times.
Care partners can support exercise plans, sometimes making it motivating to exercise together, go for walks together, or stay active as a team. They understand daily schedules and routines, helping determine what will work for the person with PD.
Care partners can assist with coaching movements using cues. “Clear, calm, very specific directions can really help someone who might be struggling to move or get around the house,” Baker said.
The physical environment also matters. Care partners can ensure that pathways around the house are wide enough, free of clutter, and well-lit. If someone needs to reach the bathroom in the middle of the night, the care partner can make sure the path and lighting support safe movement.
Questions A Physical Therapist Will Ask
At the first PT appointment, therapists want to understand how physical therapy can help in daily life. What’s important to the patient? What do they want to accomplish or improve? Is it travel or time with family? This shapes the exercise and PT program.
Physical therapists need to know what PD symptoms someone experiences and how they affect daily routine. They want to know where the person has had success with exercise in the past and what they’ve enjoyed. Understanding what helps someone participate in PT guides the program design.
Finding A Physical Therapist
Several resources can help connect people with physical therapists who understand PD:
- Neurologists are often well connected with physical therapists in the area
- State APDA chapters can connect people with knowledgeable local physical therapists
- Boston University’s exercise helpline, toll-free phone, 888-606-1688, and email at rehab@bu.edu helps answer exercise questions and can assist in finding physical therapists
- The American Physical Therapy Association website offers a searchable list of physical therapists (select neurology as the specialty)
- The APTA’s specialized section for physical therapists working with degenerative diseases including PD provides another connection point
Questions and Answers
Home Versus Outpatient Physical Therapy
Home-based PT brings the therapist to the person’s home environment. This can be particularly effective when someone struggles with situations like getting down the hallway to the bathroom. Working in the actual environment allows for realistic strategies in that specific space. Home PT requires a referral.
Outpatient PT takes place at a clinic where the person comes for appointments. This setting may provide access to different equipment and environments. Outpatient therapy works well for people who can more easily get out of the house and travel to the clinic.
Both types can be effective depending on individual needs.
Insurance Coverage And Episodic Care
While the presenters couldn’t address specific insurance questions, Baker recommended discussing insurance coverage with the physical therapist early in the first examination. Talk through any limitations that exist and get the therapist’s input on how long the course of appointments might last. The therapist may not be able to answer immediately on the first visit, but after working together, they develop an idea of the timeline based on goals.
Outpatient PT is episodic. Visits happen regularly while working together on goals, then that round of therapy, or episode of care, ends. One major goal is helping someone with PD continue exercise, activity, and safe movement after PT ends. This requires creative solutions to keep people connected with exercise.
The intent is for the person to maintain their exercises and potentially join classes during the period between physical therapy courses. Then the person returns for a new evaluation to check in, review progress using measurements from the last round, and potentially tune up the program over one or two sessions before that course ends. The physical therapist follows the person longitudinally over the long term, but PT itself won’t be continuous.
Staying Motivated Between Physical Therapy Episodes of Care
Baker acknowledged fatigue as a real barrier that people often report. For staying motivated, she emphasized that individuals know themselves best and should consider what helps them stick with plans or programs long-term.
Some people thrive with classes that have a set time and place. Others find that getting dressed, getting in the car, and driving somewhere creates too many barriers. Those people are more likely to benefit from an exercise program they can do from home.
Some people find community bonds at classes like those at local YMCAs intended for people with PD, and that social connection motivates weekly attendance. Others stay committed to step counts on their watches and want those circles to close. If tracking data and information works, that’s effective.
“Exercise is essential for people with Parkinson’s,” Baker said. Research suggests it may slow PD progression. The physical therapist’s job is to make sure each of their patients with PD understand that and help them figure out how they will keep exercising over the course of their Parkinson’s disease.
Zoeller emphasized the importance of honesty with physical therapists. When patients come in and say they didn’t do exercises that week, it opens helpful conversations. Sharing barriers like fatigue allows therapists to help problem-solve.
Should Consistent Exercisers Still See A Physical Therapist?
When asked whether someone who exercises five days a week on a consistent program should still consult with a physical therapist, Baker answered, emphatically, yes. A physical therapist can/will collect different data points to understand movement and keep metrics on file. This might be a single appointment to get baseline testing, giving the person a chance to ask questions. Perhaps one or two areas of the exercise program could use support.
If a longer course of physical therapy isn’t necessary, the person can stay continuous with their current program but return to the physical therapist next year for evaluation. The therapist can track information and potentially pick up very small changes in data before they show up significantly in daily life.
Zoeller compared it to the dental model: some people brush teeth twice daily and floss but still visit the dentist twice a year. Coming to PT while on a good exercise program doesn’t necessarily mean getting new exercises. Even patients on effective exercise programs can ensure exercises are addressing challenges like balance, and helping them fine-tune what they are doing within existing activities.
Pain As A Reason To See A Physical Therapist
Pain is sometimes a prominent and potentially underlooked symptom that people with PD experience. Sometimes pain becomes the barrier to participating in movement, walking, and exercise. This alone should be addressed, and a course of PT might be dedicated to solutions or suggestions for managing pain so the person can move better. Pain is definitely a reason to connect with a physical therapist, and managing it will benefit overall function and movement.