Vision problems are among the most common — and most under-discussed — symptoms in Parkinson’s disease, affecting everything from reading and screen use to balance and driving safety. In early April, PMD Alliance hosted a webinar in which movement disorder specialist and neuro-ophthalmologist Dr. Shahnaz Miri answered vision questions submitted by people living with Parkinson’s. She was joined by Dr. Scott Sorenson, an ophthalmology resident, who provided a talk at dry eye disease.
Key Takeaways
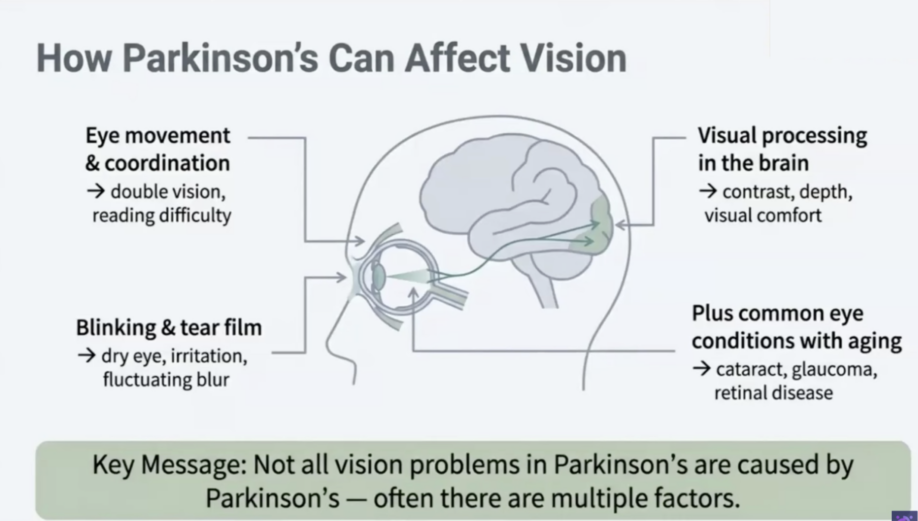
Parkinson’s affects vision in several distinct ways — and most are treatable. The disease reduces blink rate, impairs eye muscle coordination, and disrupts dopamine-dependent visual processing pathways from the retina to the brain. These mechanisms cause dry eyes, reading difficulty, double vision, reduced contrast sensitivity, and depth perception problems. Age-related conditions like cataracts, glaucoma, and macular degeneration can coexist with Parkinson’s but are not directly caused by it.
Dry eyes are extremely common and very treatable. Reduced blink rate is the primary driver. First-line interventions include staying hydrated, using a humidifier, applying artificial tears, using warm compresses, taking omega-3 supplements, and practicing the 20-20-20 rule: every 20 minutes of screen or reading time, look 20 feet away for 20 seconds. For persistent symptoms, a doctor can insert punctal plugs to help retain moisture.
Reading difficulties often have multiple causes beyond the prescription on your glasses. Reduced contrast sensitivity (text appearing washed out) and dry-eye-related blur both contribute. Recommendations include switching from progressive/multifocal lenses to single-vision reading glasses for close-up tasks, and adding a dedicated task light over reading material. These two changes alone can make a meaningful difference.
Double vision warrants a professional evaluation — and is often treatable. A simple test: cover one eye. If the double vision disappears, it is binocular and likely related to eye muscle alignment. The pattern most common in Parkinson’s — double vision or overlapping letters primarily during near tasks — is consistent with convergence insufficiency. Prism glasses, prescribed by an eye doctor, can help by mechanically compensating for the alignment problem.
Progressive lenses may be worsening your depth perception. Over 60% of survey respondents use progressive lenses. Because these lenses create different focal zones, they can add to depth perception difficulties already associated with Parkinson’s. Using single-distance glasses for walking and outdoor activities can meaningfully reduce fall risk.
Visual hallucinations are treatable and should be reported to your doctor. Many people with Parkinson’s experience visual hallucinations (seeing people, animals, or figures) but don’t mention them. These are linked to visual processing changes in the brain and can be treated with medication.
Blepharospasm (involuntary eyelid spasms or closure) can be treated with Botox® injections administered by a movement disorder neurologist or neuro-ophthalmologist. This symptom should be proactively raised with a physician.
Resources
- Webinar Recording — PMD Alliance YouTube
- Vision in Parkinson’s Disease — Stanford Parkinson’s Community Outreach
Continue reading for detailed notes,
-Elizabeth
Vision in Parkinson’s: What Concerns You Most?
Speakers:
- Shahnaz Miri, MD, MBA, movement disorder specialist and neuro-ophthalmologist; Founder and CEO of Vision Neurology Center in San Francisco, CA and Iatrion AI.
- Dr. Scott Sorenson, ophthalmology resident, University of Washington
Webinar Host: PMD Alliance
Webinar Date: April 8, 2026
Summary by: Elizabeth Wong, Stanford Parkinson’s Community Outreach
Why Vision Matters in Parkinson’s
Vision problems are among the most commonly reported yet under-discussed symptoms in Parkinson’s disease. They affect reading, screen use, depth perception, walking, stair navigation, driving, safety, and overall quality of life.
Prior to the webinar, 51 participants completed a survey about their vision concerns; nearly all reported regularly seeing an eye doctor. Survey highlights included: 88% wear glasses or contacts; 67% use progressive or multifocal lenses; 90% report difficulty focusing or reading; 76% have dry eyes; 65% experience eye pain or burning; 63% report vision-related balance difficulties; 61% experience double vision; and 35% report some form of visual phenomena.
How Parkinson’s Affects the Eyes
Parkinson’s disease affects vision through several mechanisms.
It reduces blink rate — typically 16-18 blinks per minute in the general population, but much lower in Parkinson’s (5-10 blinks per minute) — which leads to dry eyes, surface irritation, and fluctuating blurred vision.
It impairs eye muscle coordination and focusing ability, contributing to reading difficulty and double vision.
It also affects visual processing: the pathway from the retina to the brain’s visual cortex relies on dopamine, so low dopamine levels can impair contrast sensitivity and visual clarity.
Separately, age-related conditions — cataracts, glaucoma, macular degeneration — can coexist with Parkinson’s but are not directly caused by it and should be evaluated independently. Studies do show a slightly higher rate of macular degeneration in people with Parkinson’s compared to age-matched controls, though there is no direct causal relationship.
Reading Difficulties and Contrast Sensitivity
Two Parkinson’s-specific factors compound reading difficulty beyond what glasses can fix are: reduced contrast sensitivity (text appearing washed out, especially in dim light) and dry eye-related fluctuating blur. Despite having an updated prescription, many people with Parkinson’s still struggle to read because these underlying issues are not addressed by lenses alone.
Dr. Miri’s practical recommendations are:
* add a dedicated task light over reading material to improve contrast;
* treat dry eyes (see below); and
* switch from progressive or multifocal lenses to single-vision reading glasses or single-vision computer glasses for close-up tasks.
Progressive lenses are not optimal for sustained near-vision tasks in people with Parkinson’s, particularly those with convergence difficulty.
Dry Eye Disease (This portion only was presented by Dr. Scott Sorenson).
The tear film, the coating covering the eye’s surface, is a complex system; if any component — tear quantity, tear quality, blink rate, eyelid health, or drainage — is compromised, symptoms result. In Parkinson’s, reduced blink rate is the primary additional risk factor for dry eyes. Dry eyes can present as burning, itching, tearing, fatigue, double vision, or fluctuating blur.
First-line interventions include:
- Staying well hydrated
- Using a humidifier if the environment is dry
- Avoiding fans directed at the face during sleep
- Applying over-the-counter artificial tears (try different brands to find one that works)
- Using warm compresses or heat masks to stimulate the natural oil glands in the eyelids
- Omega-3/fish oil supplementation
- The 20-20-20 rule: every 20 minutes of screen or reading time, look 20 feet away for 20 seconds
For persistent or severe symptoms, punctal plugs — tiny drain plugs inserted into the tear ducts to retain moisture — and other clinical treatments are available through an eye doctor.
Double Vision and Convergence Insufficiency
Double vision should always be evaluated by an eye care professional. The first diagnostic step is simple: cover one eye. If double vision disappears, it is binocular and likely caused by eye muscle misalignment — this is the type most relevant to Parkinson’s. Approximately 50% of survey participants reported double vision or letter overshadowing primarily during near tasks, a pattern consistent with convergence insufficiency, or the inability to pull both eyes inward together for near focus. This condition is more prevalent in people with Parkinson’s, likely due to dopaminergic effects on brainstem pathways governing eye movement.
Treatment options include prism glasses, which mechanically compensate for the misalignment and reduce the eye strain caused by the constant effort to converge. However, if other contributing factors — dry eyes, cataract, macular degeneration, incorrect lens type — are not also addressed, prism alone may not be sufficient. Thyroid eye disease and nerve problems can also cause double vision and should be ruled out. Anyone experiencing double vision should begin with an optometrist or ophthalmologist, who can refer to a neuro-ophthalmologist if needed.
Depth Perception
Depth perception difficulties in Parkinson’s have two contributing causes: impaired smooth eye movement tracking, which affects the ability to judge distances across a scene, and reduced contrast sensitivity in dim light, which makes edges harder to distinguish.
Progressive lenses add a third contributing factor by creating conflicting focal zones — the upper portion of the lens is set for distance, the lower for near, which causes additional distortion when looking down.
Dr. Miri recommends using single-distance glasses for walking and outdoor activities, reserving progressives for stationary near tasks such as watching television.
Visual Hallucinations
Formed visual hallucinations — seeing people, animals, or other figures that do not exist — are reported by a meaningful proportion of people with Parkinson’s but frequently go undisclosed. They are linked to dysfunction in the occipital lobe’s visual processing centers, as suggested by PET scan data. They are treatable with medication and should be reported proactively to a movement disorder specialist. Patients are often relieved to learn these experiences are a recognized feature of the disease.
When to Seek Urgent Care
Sudden vision loss, sudden onset of large flashes of light, a “curtain” descending over the visual field, or the acute disappearance of a significant portion of the visual field are urgent symptoms unrelated to Parkinson’s that require immediate evaluation by an eye doctor. Persistent light flashes lasting several hours also warrant a prompt eye exam to rule out retinal causes.
Questions and Answers
The following questions were submitted by participants prior to the webinar.
Q: Reading has become very difficult and the pleasure of it has been taken away. Can anything help?
A: Many of the issues discussed in this webinar contribute to reading difficulty in combination — contrast sensitivity loss, dry eyes, convergence insufficiency, and incorrect lens type. To some extent these can be addressed. Switching to single-vision reading glasses, adding a task light, and treating dry eyes are good starting points. Prism glasses may also help if convergence insufficiency is a factor. It is worth working through these systematically with an eye doctor.
Q: Will Parkinson’s cause me to go blind or lose my vision progressively?
A: Parkinson’s disease itself does not cause sudden or progressive vision loss. If anyone is experiencing a gradual or rapid decline in vision, that is likely not attributable to Parkinson’s and should be evaluated separately. This is reassuring — Parkinson’s does not cause that kind of problem.
Q: I have morning tears and scratchy, irritated eyes. Is that related?
A: Yes — morning dryness, tearing, and scratchy eyes are all part of the dry eye cluster discussed in this webinar. These symptoms are managed by an optometrist or regular eye doctor and are very treatable.
Q: I am having trouble with depth perception and judging distances, especially on stairs. What can I do?
A: One practical change is switching to single-distance glasses for walking and navigating stairs, rather than progressive lenses. If double vision is also present, getting evaluated for that is an important next step.
Q: I have had multiple vitrectomies and other eye surgeries. Are these related to Parkinson’s?
A: No — prior eye surgeries and the conditions requiring them are not directly related to Parkinson’s disease. They are separate issues.
Q: I have macular degeneration. Is that connected to Parkinson’s?
A: Macular degeneration is not directly caused by Parkinson’s. Some studies show a slightly higher rate of macular degeneration in people with Parkinson’s compared to age-matched controls, but there is no direct causal relationship. These are separate conditions requiring separate management.
Q: I have been diagnosed with a vestibular schwannoma. Is that related to Parkinson’s?
A: Vestibular schwannoma — a benign growth on the vestibular nerve — is not related to Parkinson’s disease. It is a coincidental finding. People with this condition will experience additional balance difficulties and should be monitored by a neurologist. Vestibular rehabilitation through physical therapy can be helpful, and some medications can address associated nystagmus.
Q: I sometimes experience visual aura. Should I be concerned?
A: Visual aura — typically colorful or zigzag phenomena lasting 5–15 minutes — is often associated with migraine and is generally benign, particularly if it is something you have experienced for many years. However, if it is new onset, it should be evaluated by a primary care physician or neurologist, and a brain MRI may be recommended.
Q: I see light flashes. Is that a concern?
A: Brief light flashes lasting only a few seconds are not typically a major concern, though it is worth mentioning to your eye doctor to rule out a retinal cause. Persistent light flashes lasting several hours are a different matter and require prompt evaluation by an eye doctor, as they can indicate a retinal problem unrelated to Parkinson’s.
Q: I am having trouble getting a referral to a neuro-ophthalmologist. How do I find one?
A: There are approximately 600 neuro-ophthalmologists practicing in the United States. The North American Neuro-Ophthalmology Society (NANOS) maintains a directory on their website where you can search for a specialist in your area. You can ask your eye doctor or primary care physician to refer you, or use the directory to identify someone and request a referral. If a neuro-ophthalmologist is not accessible, ask for a referral to any eye doctor who evaluates and treats double vision.
Q: My doctor said my vision problems are not related to Parkinson’s. Is that true?
A: A physician saying vision problems are “not caused by Parkinson’s” typically means they cannot attribute them definitively to the disease — not that there is no association. Studies show that visual complaints are significantly more common in people with Parkinson’s than in age-matched controls: 82% of people with Parkinson’s experience some form of visual problem, compared to 48% of healthy people the same age.
Q: I use prism glasses but they aren’t helping. Why?
A: Prism addresses only one piece of the puzzle. If other contributing factors — dry eyes, cataract, macular degeneration, optic nerve disease from glaucoma, or incorrect lens type — are not also being treated, prism alone may be insufficient. A comprehensive evaluation to identify all contributing causes is recommended.
The following questions were asked live during the webinar.
Q: Can you talk about blepharospasm? My eyes close and I can’t control them, and it’s really impacting my day-to-day life.
A: Blepharospasm is involuntary spontaneous twitching and spasm of the eyelid muscles. It is associated with Parkinson’s and other movement disorders, including cervical dystonia. When it is affecting both eyes and impacting daily function, it is very treatable — Botox® injections to the eyelid muscles, administered by a movement disorder neurologist or neuro-ophthalmologist, relax the muscles and keep the eyes open.
Q: I wear monovision contact lenses — one for near, one for far. Would you not recommend that for someone with Parkinson’s?
A: Monovision works well for many people, but for someone already experiencing depth perception difficulties, it adds to the problem rather than helping. Trying conventional correction without monovision to see whether depth perception improves.
Q: I notice my eye problems are worse when I’m tired, when I don’t get a good night’s sleep, or later at night. Is that my imagination?
A: No — this is a recognized pattern. More waking hours mean more surface dryness and greater eye muscle fatigue, both of which worsen toward the end of the day. Myasthenia gravis — a rare condition involving fatigue of the eye muscles causing fluctuating double vision and eyelid fatigue that worsens as the day progresses — can coexist with Parkinson’s. If there is a consistent, pronounced pattern of worsening double vision and eyelid fatigue toward day’s end, this is worth discussing with a neurologist.