In early December, the Parkinson Foundation hosted a webinar on skin and bone health in Parkinson’s disease (PD) with neurologist Dr. Nicki Niemann, and metabolic bone disease specialist Dr. Kenneth Lyles. Dr. Niemann first discussed skin issues in PD, noting that skin disorders are common in PD but often overlooked. Dr. Lyles followed with a presentation on bone health in PD, noting that those with PD have four times higher risk of hip fractures than those without.
According to Dr. Niemann, seborrheic dermatitis is the most common skin disorder not related to treatment, occuring in 20-60% of people with PD, compared to 3-4% in non-PD people. Melanoma risk is elevated by 2-3 times, but overall cancer risk is reduced. It is important to note that levodopa does not increase risk of melanoma.
There are also skin issues related to PD treatments. Dopamine agonists often lead to leg edema, although skin-related side effects of oral medications are otherwise rare. “Invasive” therapies (infusion or DBS) can be associated with skin infection, redness, or skin erosion.
Looking to the future of skin in PD research, recent studies have shown that skin biopsy is a promising tool in the diagnosis of PD.
Dr. Niemann addressed sweating.
According to Dr. Lyles, those with PD have a two to three times higher risk of fractures than in non-affected people. This is because people with PD have lower bone density. In PD, people may also experience bradykinesia, rigidity and also may have stooped posture – all of which contribute to a higher risk of falling. Having a lower bone density and a higher risk of falling results in a higher risk of fractures.
Additionally, it is known that exercise and movement keeps the bones strong. People with PD may not move as much. The lack of activity can increase the amount of bone loss that occurs.
Risk factors for osteoporosis include increasing age, smoking, excessive alcohol, and family history of fractures, loss of height, and prolonged glucocorticoid use. There are also secondary risk factors such as taking PPIs, anticonvulsants, aromatase inhibitors and steroids. Additionally, having epilepsy, multiple sclerosis, PD, celiac disease, cystic fibrosis, diabetes and others are also secondary risks.
There are multiple treatments for osteoporosis, such as stopping smoking, limiting alcohol, and avoiding sedating medication. Starting weight bearing activities, physical therapy and exercise, and proactively preventing falls, as well as maintaining calcium and vitamin D levels are also helpful. Medication treatments such as some hormonal treatments, antiresorptive medications, and anabolic medications can also be prescribed.
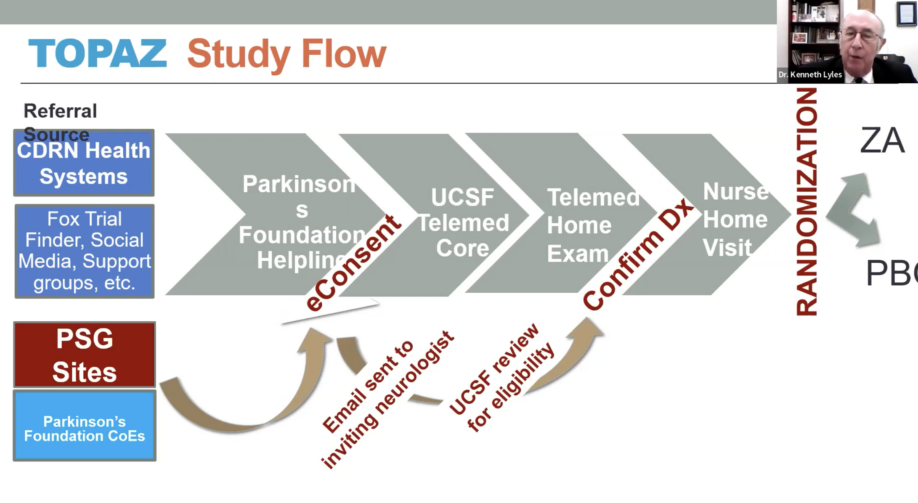
Finally, Dr. Lyles provided an overview of the TOPAZ trial, which uses a drug called Reclast (zoledronic acid) given in an IV format to determine if it suppresses bone turnover and bone loss. If you have a hip fracture and you are over the age of 50, you have a 25% chance of another fracture in the next 24 months. This makes maintaining bone density very important. Randomized trials in other populations show a 30-35% reduction in clinical fractures with the effect lasting at least 2 years, and 28% decreased mortality. The TOPAZ trial is available for US residents, and can be done from home as nurses come to the participant’s home. For more information or to take part in the TOPAZ trial, please contact the trial organizers:
- Phone: 1-800-4PD-INFO (473-4636)
- Website
For more information on fall prevention, please see this Stanford Parkinson’s Community Outreach webpage:
For a recording of this webinar, please see this Parkinson Foundation YouTube webpage
See my notes below of the December 1st webinar.
Regards,
– Joëlle Kuehn
“Skin and Bone Health in Parkinson’s Disease” – Webinar Notes
Speakers:
- Kenneth W. Lyles, MD, Professor of Medicine, Duke University Medical Center, Durham, North Carolina
- Nicki Niemann, MD, neurologist, Barrow Neurological Institute, Phoenix, Arizona
Webinar Host: Parkinson Foundation
Webinar Date: December 1, 2021
Summary by: Joëlle Kuehn, Stanford Parkinson’s Community Outreach
Session 1: Parkinson’s disease and skin – Dr. Nicki Niemann
Skin disorders not related to treatment:
- Melanoma:
- Cancer & PD:
- If you have PD, your overall risk of cancer is reduced
- However, the risk of skin cancer, especially melanoma, is increased
- Melanoma is a skin cancer arising from pigmented cells
- Risk of melanoma is 2-3x higher after PD has started to manifest and has been diagnosed:
- No increased risk before diagnosis of PD
- The association is poorly understood
- There are a lot of shared risk factors which could contribute to the association:
- Age, male, caucasion, red hair, fair skin, pesticide exposure
- Shared pathological, genetic, pathophysiological and imaging features:
- Ex. alpha-synuclein is found in a melanoma biopsy as well
- Ex. certain genes that cause skin pigmentation also regulate risk of melanoma and PD
- Ex. genetic PD can be found mutated if you analyze tumor cells from a melanoma
- Levodopa does not increase risk of melanoma
- Tips to reduce risk of melanoma: visit your dermatologist annually, reduce direct sun exposure, use sun block:
- Check your own skin:
- Melanomas can be identified by “ABCDE”
- Asymmetry
- Border – irregular border
- Color – color variability
- Diameter – greater than ¼ inch
- Evolution – changes over time
- Check your own skin:
- Cancer & PD:
- Seborrheic dermatitis (SD):
- Condition isn’t diagnostic of PD to any extent, but may help raise suspicion of PD
- Can range from mild (not even noticeable) to very severe (impacts quality of life)
- Core symptoms: itching, scaling, redness, and burning in sebaceous areas:
- Scalp, hairline, around nose, chest, around mouth
- Studies estimate 20-60% of people with PD may have this condition:
- Compared to 3-4% in non-PD people
- Theories to explain the association:
- Reduced facial movement (can cause sebum buildup)
- Immune dysfunction
- Autonomic dysfunction
- Changes in skin yeast species in PD
- Treatment and Tips:
- Usually very easy to treat
- Most common is over the counter topical treatment – shampoo – ketoconazole 1-2%
- If it doesn’t work, go see a dermatologist
- Topical:
- Salicylic acid
- Shampoos (zinc, selenium, tar, ketoconazole 1-2% (most common)
- Steroids
- Other immunosuppressants
- Systemic antifungals
- Disorders of sweating:
- Increased sweating is seen prior to diagnosis and manifestation of PD
- Increased sweating is more common than reduced sweating
- Why do changes in sweating occur?:
- PD: may be related to “Autonomic” dysfunction (disorders of the autonomic nervous system – blood pressure, digestion, sweating), and possibly also medications (ex. antidepressants)
- PD is not the only reason someone can develop problems
- Just because someone has symptoms, and PD, doesn’t mean they are related
- Non PD related: other medications, cancer, endocrine condition (increased thyroid function, increased metabolic rate), infection, sleep apnea
- Increased sweating: Head, neck, trunk:
- Typically during medication “OFF” state, or when you are too “ON” (especially if “ON” state is with dyskinesias):
- Medications are at peak function at ON state
- Typically during medication “OFF” state, or when you are too “ON” (especially if “ON” state is with dyskinesias):
- Treatment:
- PD: adjust PD medications (reduce OFF time, reduce dyskinesia), review medication list, DBS, Botox (localized sweating)
- DBS leads to a reduction of off times, and reduction of dyskinesias, so it can indirectly reduce sweating
- General recommendations:
- Light clothes, like-warm/cold showers, drink cold liquids, antiperspirants, dress shields, avoid triggers, non-synthetic shoes, etc.
- Medications:
- Don’t often prescribe medication
- Propranolol, topical treatments (glycopyrrolate [Qbrexza], aluminum chloride, iontophoresis)
- PD: adjust PD medications (reduce OFF time, reduce dyskinesia), review medication list, DBS, Botox (localized sweating)
- Reduced sweating:
- Often medication-related (anticholinergics, trihexyphenidyl, amantadine, glycopyrrolate)
- Often medication-related (anticholinergics, trihexyphenidyl, amantadine, glycopyrrolate)
- Others:
- Rosacea:
- Redness of central face (cheeks and nose), and “phymatous” changes (increased thickness and nodularity of skin, especially nose)
- If someone has a diagnosis of rosacea, the risk of PD is 2x
- Bullous pemphigoid:
- Itching, redness, fluid-filled blisters
- Problem is that blisters can break, and can increase risk of skin infection, which can lead to a blood-borne infection and that can be very dangerous
- High mortality risk
- Increased risk with many neurological disorders (not just PD)
- 50% of people with this condition also have a neurological condition
- Perioral dermatitis:
- Redness and skin breakdown around the mouth due to uncontrolled drooling
- Easily treatable with botulinum toxin injections into the salivary glands
- Rosacea:
Treatment-related skin disorders:
- Oral medications:
- Carbidopa/levodopa (equivalent to levodopa/benserazide):
- Can cause diffuse rash: likely due to yellow dye in tablet (Sinemet 25/100 formulation):
- Very rare
- Tip: switch to different formulation (10/100, 25/250, Parcopa, Stalevo, Sinemet CR) if the side effect occurs
- Very few reports of true allergy to levodopa and carbidopa, more likely allergic to the dye in that specific formulation
- Levodopa does not increase risk of melanoma
- Can cause diffuse rash: likely due to yellow dye in tablet (Sinemet 25/100 formulation):
- Amantadine:
- Can cause leg swelling (edema):
- Commonly overlooked problems
- Many PD medications can cause leg edema, primarily amantadine
- Livedo reticularis (8-40%):
- Not a rash but skin has a web-like appearance
- Due to changes in blood flow through the skin
- Not dangerous but isn’t cosmetically pleasing either
- Can cause leg swelling (edema):
- Dopamine agonists: ropinirole, pramipexole, rotigotine, apomorphine:
- Causes leg swelling
- If didn’t have leg swelling, and then a few months later they do develop leg swelling, most likely culprit is PD medication. Unlikely to be heart or lung problems
- Leg swelling happens in 11-42% of PD patients
- Typically if offending medication is stopped, it’ll go away within a few weeks to a few months
- Water pills/diuretics treatments don’t work well, rather resolve with drug discontinuation
- Carbidopa/levodopa (equivalent to levodopa/benserazide):
- Medication infusion and DBS:
- Levodopa-carbidopa intestinal gel (Duopa):
- What it is: medication administered through feeding tube (PEG-J) 24/7
- Infection risk around tube (happens in 12.9 – 20% of cases)
- Redness (16%), leakage around stoma (the opening in stomach), and abscess
- Tips: ensure proper PEG-J care is taking place, and an increased access to healthcare providers can help mitigate or prevent side effects
- Subcutaneous infusion of levodopa/carbidopa (trialed in US), and apomorphine (approved in Europe):
- What it is: medication administered through a patch with a 6-9mm needle attached to it. Non-surgical
- Localized skin reactions: redness, skin infection, abscess, nodules, pain
- Tips: rotate the site, keep good hygiene, massage, regular ultrasounds
- Deep brain stimulation (DBS):
- What it is: implantation of electrical wires into the brain, connected to a pacemaker-like battery in the chest, for treatment of PD motor symptoms
- Skin-related complications are not common, but they exist:
- Hardware infections (5%): Can be treated with antibiotics, but if it persists, removal of the entire system may be necessary
- Skin erosion:
- Can see device through the skin as it thins out over time
- From battery, the extension wire behind site, burr hole site
- It is extremely rare
- Tips: treatment/prevention is entirely healthcare provider-dependent
- Levodopa-carbidopa intestinal gel (Duopa):
Skin in the diagnosis of PD:
- What is alpha-synuclein: Small protein essential for cellular function, present all over the body
- Alpha -synuclein clumps together and accumulates in the brain in PD
- Recent research shows: alpha-synuclein can be detected in both the brain (after death), but also in the body (during life)
- A biopsy of non-brain tissue (such as skin) might help confirm/support a diagnosis of PD:
- What research shows:
- Skin biopsies are helpful when positive (good at identifying only people with PD; high “specificity”)
- Skin biopsies are not always helpful when negative (can be negative even in people who do have PD; low “sensitivity”)
- Role of skin biopsies in the future:
- Likely helpful when clinical diagnosis is uncertain
- Enrich trial results
- Further study needed before it becomes standardized
- May not discriminate well between parkinsonian disorders
- What research shows:
Session 2: Bone health in Parkinson’s – Dr. Kenneth Lyles
Impact of osteoporosis:
- By 2020, about 12.3 million in US are expected to have osteoporosis, and over 45 million with low bone mass
- More than 280,000 hip fractures yearly in older adults
- 20-30% of hip fractures in older adults die within 1 year
- Cost of fractures from osteoporosis and low bone mass will be $25 billion/year by 2025
- Number of osteoporotic fractures yearly (over 2 million) exceeds incidence of heart attack, stroke, and breast cancer combined
- In women 55 and older, cost of fracture care exceeds cost of heart attack, stroke, and breast cancer combined
PD and fractures:
- PD patients have a higher risk of fractures and disability:
- If you have PD and have fractures, you have more disability
- Having PD increases risk of having a fracture
- Impact of fractures in patients with PD:
- Fractures occur 2-3 times more frequently in patients with PD than occur in non-affected people
- Hip fractures occur 4 times more frequently
- At best, less than 5% of PD patients with fractures are treated
- After fractures, patients with PD will have more functional disability and take longer to recover from their injury with a risk of worsening symptoms, loss of independence and cognitive decline
Screening for osteoporosis:
- Investigate any bone fracture
- Annual height measurement without shoes, history of falls
- DEXA testing should be consider for:
- Women age 65+
- Women post-menopausal age 50-64 with risk factors
- Men age 70+
- Men age 50-69 with risk factors
- Vertebral Imaging:
- ⅔ fractures in spine never come to medical attention
- Considered for:
- Women 70+
- Men 80+
- If there is a height loss greater than 4cm
- Patient with history of vertebral fracture
Risk factors for osteoporosis:
- Primary risk factors:
- Increasing age
- Female
- Family history of fractures or osteoporosis
- Smoking
- Excessive alcohol intake (more than 2 drinks/night for women, 3 drinks/night for men)
- Low body weight (under 100 pounds at age 18-25)
- History of low impact fractures
- Loss of height/presence of kyphosis
- Prolonged glucocorticoid use (although effective in treating multiple diseases, there are risks)
- Secondary risk factors:
- Medications: PPIs, anticonvulsants, aromatase inhibitors, tamoxifen, Depo Provera, steroids, etc.
- Neurologic: epilepsy, stroke, multiple sclerosis, Parkinson’s disease
- GI: inflammatory bowel disease, celiac disease, gastric bypass
- Rheumatologic problems: RA, systemic lupus, ankylosing spondylitis
- Genetic issues: cystic fibrosis, Ehlers-Danlos, etc.
- Endocrine: diabetes
- Hypogonadal state: premature menopause (<40 yo), androgen loss/insensitivity
- Chronic diseases: ESRD, COPD, HIV, etc.
Making the diagnosis of osteoporosis:
- Measure osteopenia or low bone mass
- Measure through tests such as DEXA or FRAX
- Osteopenia: DEXA score of -1.0 to -2.5
- Osteoporosis: DEXA score of ≤ -2.5
Non-prescription treatments:
- Stop smoking, limit alcohol, avoid sedating medications
- Start weight bearing activity, fall prevention, hip protectors, physical therapy, regular exercise
- Vitamin D levels maintained > 30 ng/ml
- Vitamin D3 preferred (fatty animal source); D2 is plant based (is vegetarian)
- Calcium for women (51+ years), and males (71+): 1000mg per day:
- Limit any single dose to no more than 500-600 elemental calcium
- Split dose if needed
Medication treatments:
- Hormonal medications: estrogen, raloxifene
- Antiresorptive medications: bisphosphonates, denosumab
- Anabolic medications: teriparatide, abaloparatide, romosozumab (has both anti-resorptive and anabolic impact)
TOPAZ (Trial of Parkinson’s and Zoledronic Acid) study:
- Use a drug called Zoledronic acid, a.k.a. Reclast which if given IV suppresses bone turnover and bone loss
- If you have a hip fracture and you are over the age of 50, you have a 25% chance of another fracture in the next 24 months
- Randomized trials in other populations show a 30-35% reduction in clinical fractures (1 shot per year)
- Effect lasts at least 2 years, 100% persistence
- Trial after hip fracture: 28% decreased mortality. Not only reduce fractures, but also reduced mortality
- Nurses come to patients home:
- Registered nurses
- Good Clinical Practice certified
- Are very knowledgeable about the TOPAZ study
- TOPAZ study is accepting new patients – in US only
- For more information/to take part:
- Phone: 1-800-4PD-INFO (473-4636)
- Website: topazstudy.org
Question & Answer
Question: Is there a PD safe treatment for night sweats?
Answer (Dr. Niemann): It comes down to pinpointing why it is happening at night. The most likely reason why it’s happening at night for most people with PD is because at night they aren’t taking medications, so they may take their last dose of carbidopa levodopa at 6pm, and then won’t take anything until 7 or 8 the next morning. They are effectively off all night long. If that is the case, I would add on a low dose of an extended release carbidopa levodopa at bedtime. This would be either Rytary or Sinemet Controlled Release. If you can’t control night sweats, different types of material for sheets can help. Satin sheets are recommended for people with PD, as it also helps them with turning over at night.
Question: How can Vitamin D impact bone health? What are some potential supplements one could buy at a local drug store?
Answer (Dr. Lyles): If you have celiac disease, or a gastric bypass, work with your provider to ensure blood levels are checked. D3 is the one we prefer, D2 is the plant version, it may be less effective. Most people have no trouble getting vitamin D3 at drug stores.
Question: What about collagen, calcium or other supplements?
Answer (Dr. Lyles): If you have osteoporosis or had a fracture, we think you need extra calcium, but we are sensitive to the fact that the pills are large and PD can give you swallowing troubles, so you may need to break the pill or get a chewable form. You can also use dairy products. A glass of milk has about 250 mg of calcium. People will need a total intake of 1200 mg of calcium every day. Your diet should have 500mg, so fill the remaining 700 with various methods.
Question: If someone has PD, and has skin cancer, is there anything they should let their treating physician know about PD that may impact their care, or is it something that needs to be treated independently of their PD?
Answer (Dr. Niemann): I think it is something that can be treated independently of their PD. Sometimes people say their dermatologist told them to ask me about levodopa, but the truth is that levodopa really does not increase the risk of cancer or a worse outcome or cancers.
Question: As some people age, their skin becomes more fragile and prone to abrasions, and lotions or products like vaseline may not help for some people. What are some tips for your patients regarding topical approaches to good skin health?
Answer (Dr. Niemann): It’s important to make sure you aren’t putting yourself at risk of your skin drying out, such as using alcohol-based products like cologne, some deodorants, or some hand sanitizers as well. I recommend fatty emollients, so fatty lotions that can be applied to any part of the body. It’s rare where I see a patient where those simple interventions don’t work, but in those situations I refer the patient over to the dermatologist for more specialized care.
Question: Can conditions that impact the skin also impact hair and nails? Do you have any recommendations on what to do about that?
Answer (Dr. Niemann): I’ve found fatty lotion and gentle shampoo works wonders to avoid drying out the scalp and hair.
Question: Are there any food or medications that can negatively affect bone health?
Answer (Dr. Lyles): Alcohol can be a huge thing that impairs you. Some of the medications we use to help you sleep increase the risk of falls. Some of the medicines you take for depression can cause falls. Taking the medications are important, so be aware that you have to adapt, such as walking slower at night. Don’t have rugs that can be slippery. Regarding drugs or food, I don’t think there are any that should concern you. Caffeine used to be a concern, because it causes a small amount of calcium loss, but if you put milk in the coffee, you won’t have the problem.
Question: If someone is looking to get a hip replacement, are you anticipating any difficulties for a person with PD?
Answer (Dr. Lyles): If you are thinking about a hip replacement because you have arthritis and need a hip, you should go ahead and get that. It may take longer for you to do the rehab because you may have difficulty with movement and getting about. It is important to get treated for any hip issues.
Question: Do people fall because they’re old or specifically more because they have PD?
Answer (Dr. Lyles): We know that people with PD have lower bone density, and also get stooped posture. This may not cause fractures per se, but if you have a lower density and you fall, you will have fractures. Exercise keeps the bones strong. People with PD don’t move as much, and the lack of activity can increase the amount of bone loss that occurs.
Question: Is the TOPAZ trial for US residents only or can people in Canada and Europe participate?
Answer (Dr. Lyles): As of right now, you need to be in the United States.
Question: If someone is already participating in a clinical trial, it may be observational or online, can they still participate in TOPAZ?
Answer (Dr. Lyles): If they are receiving medication it may not be possible, observational I would think so, but we need to respect other colleagues doing trials, so they are the first ones to ask. We have people available at all times on the TOPAZ side who can answer that question. In the TOPAZ trial, we can go to anyone in the US, the trial nurses will meet you where you are at. Patients don’t have to leave home to get it.