In February 2022, the American Parkinson Disease Association’s (APDA) Virginia chapter hosted a webinar on neuropsychology with neuropsychologist Dr. Michael Shapiro. Dr. Shapiro discussed cognitive and psychological symptoms of PD. He described the neuropsychological evaluation process, testing, and possible treatments.
PD is a whole body disorder, with physical, sleep, cognitive, autonomic and psychological symptoms. Neuropsychology focuses on cognitive and psychological symptoms:
- Cognitive symptoms may affect attention, processing speed, language, executive function, learning, memory and spatial abilities. There are some medications for cognitive decline although most treatments are reserved until there is more severe impairment such as dementia. In this case, memory medications such as cholinesterase inhibitors and glutamatergic agents can be useful.
- Psychological symptoms include depression, apathy, anxiety, impulse and control disorders, psychosis, hallucinations and delusions. There are some treatment options available for psychological symptoms. Depression and anxiety are often treated with SSRIs, SNRIs, anxiolytics, or rTMS. Psychosis is treated with antipsychotics. Psychotherapy may also be an effective treatment option.
In addition to the different symptoms, Dr. Shapiro also discussed ways to prevent cognitive decline such as limiting cerebrovascular risk factors. This may include managing weight and other conditions such as diabetes, exercise, diet, sleep concerns. Another way is to stay socially and cognitively active by using your brain, being social, and maintaining relationships. Finally, cognitive rehabilitation and maintenance such as speech therapy can be helpful.
For more information on psychological symptoms, please see these Stanford Parkinson’s Community Outreach webpages:
For more information on cognition, please see this Stanford Parkinson’s Community Outreach webpage:
For a recording of this webinar, please see this APDA Virginia YouTube webpage
See my notes below of the February 25th webinar.
Regards,
– Joëlle Kuehn
“Neuropsychology of Parkinson’s disease” – Webinar Notes
Speaker: Michael Shapiro, PhD, neuropsychologist, Central Virginia VA Health Care System, Richmond, Virginia
Webinar Host: APDA Virginia Chapter
Webinar Date: February 25, 2022
Summary by: Joëlle Kuehn, Stanford Parkinson’s Community Outreach
Clinical neuropsychology:
- What is it: takes the brain out for a test drive, do a status report and coordinate with other team members to create a treatment
- Brain-behavior relationship:
- How the brain functions under ideal situations and on day to day levels, but also how it functions when insults, injuries or changes occur
- Ex. if you are sleep deprived or under the influence of alcohol, your brain will not operate optimally
- Ex injury: concussion, traumatic brain injury, multiple sclerosis, PD
- Ex. if you are sleep deprived or under the influence of alcohol, your brain will not operate optimally
- Changes looking for: how the body works, emotions work, mind works
- Evaluating cognitive functioning and psychological function. Severity of symptoms and the impact on life of each symptom
- How the brain functions under ideal situations and on day to day levels, but also how it functions when insults, injuries or changes occur
- What do we do:
- No poking, prodding, machines for the most part
- In-office visit
- Lengthy (from a few hours to 8 hours)
- Thorough evaluation in terms of interview to get a background to see what life factors contribute to who you are today: education, job, medical history related to PD, mental health history
- Hours of testing to see how different areas of brain work:
- Memory, thinking speed, language abilities
- This helps to look for your patterns of peaks and valleys, strengths and weaknesses, and see how they fit together
- Many things going on in an individual that might impact the way they do testing
- Sleep, depression, medication for PD, changes in brain due to PD
- Memory, thinking speed, language abilities
- No poking, prodding, machines for the most part
- When to seek a referral:
- Anytime
- Earliest concern of a behavior change: mood, temperament, delusions, hallucinations, memory torules, mentally not feeling as sharp
- At worst, you don’t have any problems and th test can be used as a baseline for the future to see if anything changes
- Could be case where seeing symptoms of a cognitive basis before the diagnosis of PD is made
- Anytime
- How can we help:
- We get to learn a lot about you, your family structure, and what concerns you have, and how they are affecting your life
- Get a better understanding of cognitive strengths and weaknesses, and what recommendations we can make to improve quality of life
- Connect with other services, psychiatric care, communicating symptoms to neurologists who haven’t had the time, deep brain stimulation surgeries, treatment such as therapy, cognitive remediation etc.
- We get to learn a lot about you, your family structure, and what concerns you have, and how they are affecting your life
Parkinson’s Disease:
- A whole body disorder
- Physical: tremor, bradykinesia, rigidity, postural instability. Main symptoms we are treating are physical
- Sleep disturbances: REM sleep behavior disorder, apnea, disrupted sleep cycle
- Cognitive: memory, attention, language
- Autonomic: bladder, hypotension, ED
- Psychological: depression, apathy, impulsivity, compulsivity, psychosis
- Physical: tremor, bradykinesia, rigidity, postural instability. Main symptoms we are treating are physical
- Neuropsychologist focuses on cognitive and psychological
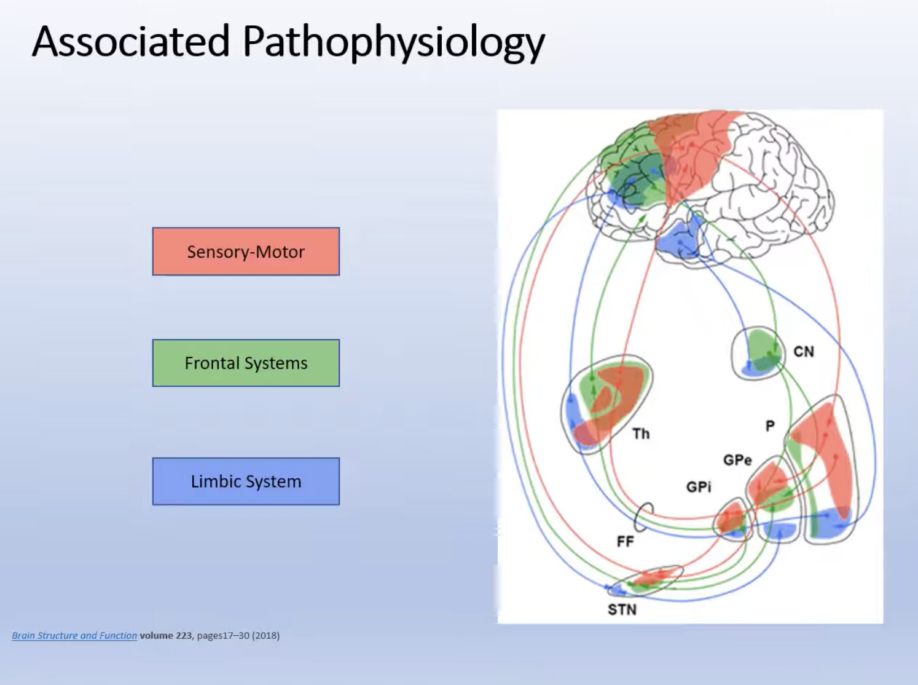
- PD’s associated pathophysiology: sensory-motor, frontal systems, and limbic systems
Psychological symptoms of PD:
- Psychological symptoms are more impactful on quality of life than physical symptoms
- Can be a function of changes neurologically to the brian, or a reaction to the changes in the body and the way the body is working. The disorder itself or the response to the disorder
- Depression:
- A primary psychological symptoms of PD
- Up to 50% of individuals with PD
- Can happen at a point in the diagnosis
- Spectrum of symptoms:
- Low mood, reduced interest in activities, hopelessness, suicidal thoughts
- Fatigue, sleep/appetite disturbances, physical slowness
- Reduced attention, brain fog, speed of thinking, memory difficulties
- Low mood, reduced interest in activities, hopelessness, suicidal thoughts
- A primary psychological symptoms of PD
- Apathy: Lack of motivation to engage in activities, decreased amount of activity in or caring about things, not being bothered by things as much, slowness to initiate movements
- Anxiety:
- Also up to 50% of individuals at some point
- Excessive worry, phobias, restlessness, avoidance, panic
- Also up to 50% of individuals at some point
- Impulse and control disorders:
- Compulsive/pathological gambling
- Buying/shopping
- Eating disorder
- Obsessing over medication taking
- Repetitive behavior (i.e. humming, tapping, taking things apart)
- Can be associated with PD (changes in dopamine) or medications such as dopamine agonists
- Can be difficult to evaluate/treat due to hesitancy to report, can be embarrassing to have to admit to
- Can be treated with a change in medication dose
- Compulsive/pathological gambling
- Psychosis:
- Hallucinations:
- Illusions/misperceptions: I.e. seeing a face in a tree
- “Presence” or “passage” hallucinations: Saw someone walk by in my periphery
- Well-formed images, objects, animals (typically non-threatening): There was someone outside
- Illusions/misperceptions: I.e. seeing a face in a tree
- Delusions (less common):
- Jealousy
- Spousal infidelity
- Paranoia
- Jealousy
- Misidentification syndromes:
- Less common
- Capgras and Fregoli syndromes
- Typically seen in the presence of dementia
- Less common
- Hallucinations:
Cognitive symptoms:
- Examples: If a person with PD says “I can’t focus on anything”, “I keep losing my train of thought”, “Why did I come into the kitchen?”, “I don’t remember you telling me that”
- Domains impacted by PD:
- Attention/working memory: ability to concentrate on what you are doing, i.e. if given a phone number and go to write it down, it’s not in your memory yet, this is considered working memory
- Processing speed: ability to think as rapidly as you used to
- Language: finding the words, thinking of the names of objects or misnaming things
- Executive functioning: frontal lobe being in charge to all other abilities, problem solving ability, ability to see things from multiple angles or perspectives, quickly organize new information
- Learning/memory
- Spatial abilities
- Attention/working memory: ability to concentrate on what you are doing, i.e. if given a phone number and go to write it down, it’s not in your memory yet, this is considered working memory
Neurocognitive change is along a continuum:
- Subtle changes that predate motor symptoms and/or PD diagnosis
- Mild neurocognitive disorder
- Previously known as mild cognitive impairment (MCI)
- Lower than baseline but not impacting day-to-day functioning abilities
- Previously known as mild cognitive impairment (MCI)
- Major neurocognitive disorder (aka dementia)
- Due to PD
- Grades of dementia from mild to severe, but dementia means a decline in cognitive abilities that affects day-to-day functional abilities. Difficulty being independent
- Dementia with Lewy bodies: Separate but related to Lewy body dementia
- Due to PD
What should I expect:
- Data varies but estimates suggest:
- Up to 30% of newly diagnosed individuals show some level of cognitive impairment
- Between 20-50% of PD patients experience cognitive impairment
- Up to 30% of newly diagnosed individuals show some level of cognitive impairment
- Difficult to use the 20-50% percentage because there are many factors
- Factors that may change these percentages and makes this less than straightforward:
- Age of onset
- Physical symptom presentation
- Regions of brain most impacted
- Medications
- Other health issues (vascular, diabetes, thyroid, sleep disturbances)
- Psychological well-being
- Age of onset
- There is some evidence of two sets of symptoms, based on onset years or duration called cluster pairing:
- This is not a given, it is still in the research phase
- Younger age of onset (50s or 60s or even younger):
- “Frontal-executive” symptom cluster
- Greater bradykinesia
- Possible that it is less likely to lead to dementia
- “Frontal-executive” symptom cluster
- Later life onset/longer disease duration:
- Posterior brain region involvement
- More memory and spatial difficulties
- Greater postural instability/gait issues
- Likely higher risk of dementia
- Motor symptoms have lower response to medication
- Posterior brain region involvement
- This is not a given, it is still in the research phase
Preventative measures for cognitive decline:
- Limit cerebrovascular risk factors:
- Heart and body health = brain health
- Exercise, eat a balanced healthy diet (i.e. Mediterranean diet)
- Manage weight, diabetes, sleep apnea
- Take control of substance use/abuse
- Heart and body health = brain health
- Stay socially and cognitively active. Using your brain, being social, maintaining relationships
- Cognitive rehabilitation/maintenance:
- Ex. speech therapy
- Strengthen existing cognitive strengths instead of focusing on the negatives
- Ex. speech therapy
Treatment for psychological symptoms:
- Depression/anxiety:
- SSRIs:
- Escitalopram (Lexapro)
- Citalopram (Celexa)
- Paroxetine (Paxil)
- Fluoxetine (Prozac)
- Escitalopram (Lexapro)
- SNRIs such as Venlafaxine (Effexor)
- Anxiolytics (benzodiazepine)
- rTMS: non-medication treatment
- SSRIs:
- Psychosis:
- Antipsychotics such as Quetiapine (Seroquel)
- Antipsychotics such as Quetiapine (Seroquel)
- Psychotherapy:
- Individual
- Group
- Family
- Individual
Pharmacological considerations for cognitive decline:
- Not a lot of great medication options
- Most treatments are reserved until more severe impairment such as dementia
- Possible SNRIs (i.e. Atomoxetine) to increase attention and executive function can be tried earlier
- Memory:
- Cholinesterase inhibitors:
- I.e. Donepezil (Aricept), Galantamine (Reminyl), Rivastigmine (Exelon)
- Exelon has a positive impact on global cognition as well as mood and activities of daily living
- I.e. Donepezil (Aricept), Galantamine (Reminyl), Rivastigmine (Exelon)
- Glutamatergic agents:
- Memantine (Namenda)
- Memantine (Namenda)
- Cholinesterase inhibitors:
Question and Answer
Question: Are diminished spatial abilities a part of neuropsychology, such as driving a car?
Answer: People may have difficulty judging the distance between two things, or the spatial nearness, farness, arrangement, and depth perception. The ability to draw a clock can become distorted. This can impact driving abilities, but also bumping into things in the home. It is along a continuum.
Question: What is the difference between Alzheimers and PD?
Answer: That becomes easier to see in some of the earlier stages, because individuals with Alzheimer’s rarely have the physical symptoms of PD. Memory can help us differentiate. In Alzheimer’s they have a flat learning curve, which is poor or inefficient learning, with rapid forgetting of information and poor ability to distinguish or recognize it later. In PD, they have a more efficient learning pattern, but still not to the degree that they are used to, and they do show difficulties spontaneously recalling as well. The difference is for PD, the strong ability to recognize information is there, it shows that the information is still in there, getting it out is the difficulty.
Question: What can I do to exercise my cognition? Is Worlde a good exercise?
Answer: Wordle, crossword puzzles are a great option, but it’s important to match the exercises to the current ability. I also suggest Pictionary with your family, or quizzing, something that will make you think and remain cognitively engaged and active.
Question: Is there self-awareness of cognitive decline or is the family member more likely to identify the changes?
Answer: Both, although sometimes it can be subtle. Usually people will notice things are becoming more difficult, or they notice their spouses or family members saying something along that. As impairments get more progressed, they can be less able to identify them.
Question: What are the effects of Zoloft and other antidepressants on cognitive functioning?
Answer: Usually very little. If we are able to relieve symptoms of anxiety and depression, it may lead us to a better ability to concentrate and pay attention. This may feel “I am feeling more cognitively acute and accurate”. They don’t improve cognitive ability in and of themselves, it’s more of a byproduct of fixing the depression or anxiety.
Question: What are your thoughts on the use of THC for anxiety relief?
Answer: It works for some people. Depending on how you consume it, THC may worsen anxiety in some people. It may fix anxiety but can introduce attention and memory problems while under the influence.