On April 6 Parkinson Society British Columbia (PSBC) hosted a 90-minute webinar on Eye Health and Parkinson’s. Neuro-ophthalmologist Jason Barton, MD, PhD, spoke for nearly an hour, staying to answer several questions afterward.
He discussed common eye conditions that may develop with aging, Parkinson’s Disease, and parkinsonism disorders and how Parkinson’s-related eye issues may be treated to improve the quality of life for people with these neurodegenerative disorders.
Dr. Barton is a good speaker. He explains things clearly. It is good to know that optometrists and ophthalmologists can treat many of the vision issues common to Parkinson’s disease. And in particular, that optometrists have plastic prism lenses that can be stuck onto your regular glasses to determine if prescription prism glasses will help with double vision or gaze palsy.
The webinar is available on the PSBC YouTube channel.
The Stanford Parkinson’s Community Outreach Program has more information about Vision and PD.
And now, on with my notes…
– Denise
“The Eye and Vision in Parkinson’s Disease” – Webinar Notes
Speaker: Jason Barton, MD, PhD, University of British Columbia
Moderator: Alana Dillon, Parkinson Society British Columbia
Webinar Host: Parkinson Society British Columbia
Webinar Date: April 6, 2022
Summary by: Denise Dagan, Stanford Parkinson’s Community Outreach Program
Overview of Today’s Talk:
A. Ocular Surface Problems (the front of the eye)
- Dry eyes
- Blepharitis
B. Vision in Parkinson’s Disease (PD)
- Retina
- Brain / Visual cortex
- Hallucinations
C. Eye Movements in Parkinsonism (cousins of Parkinson’s disease)
- Convergence insufficiency
- Square wave jerks
- Vertical gaze palsy
- Ocular dyskinesia (side effect)
D. Are eye movements helpful in diagnosis? (Dr. Barton was asked by the host to include this topic.)
A. Ocular Surface Problems
Very common, not only in people with PD (up to 7% of women over age 40).
You don’t need to see an ophthalmologist to manage dry eye effectively. Most optometrists are very good at managing dry eye.
1. Dry eye
Cause: Reduced tear formation (due to bleharitis = inflammation of the glands that produce the oily part of tears) and reduced blinking due to Parkinson’s disease
Symptoms:
- Burning, gritty sensation (may feel like you have something in your eye)
- Reflex tearing (in response to corneal pain, a reflex causes the lacrimal gland to secrete watery tears)
- Blurry vision as the cornea dries and loses its smooth glass-like quality
Signs: With dyes and the slit lamp magnified view, clinicians can see
- Abnormal break up of the tear film
- Small erosions of the cornea that stain
Treatment: (in order of progression)
- Artificial tears as frequent as needed
- Available over-the-counter
- Try to use tears with more gel-like qualities, they will last longer. The pharmacist may help you identify these.
- Protective gel at bedtime
- Available over-the-counter
- Particularly helpful if you wake up with burning irritated eyes. This may mean that your eyes don’t close properly when you sleep.
- Can also be used during the daytime. Feels like vaseline in your eye, but with a few blinks your vision will clear. Dr. Barton uses this bike riding in a strong wind.
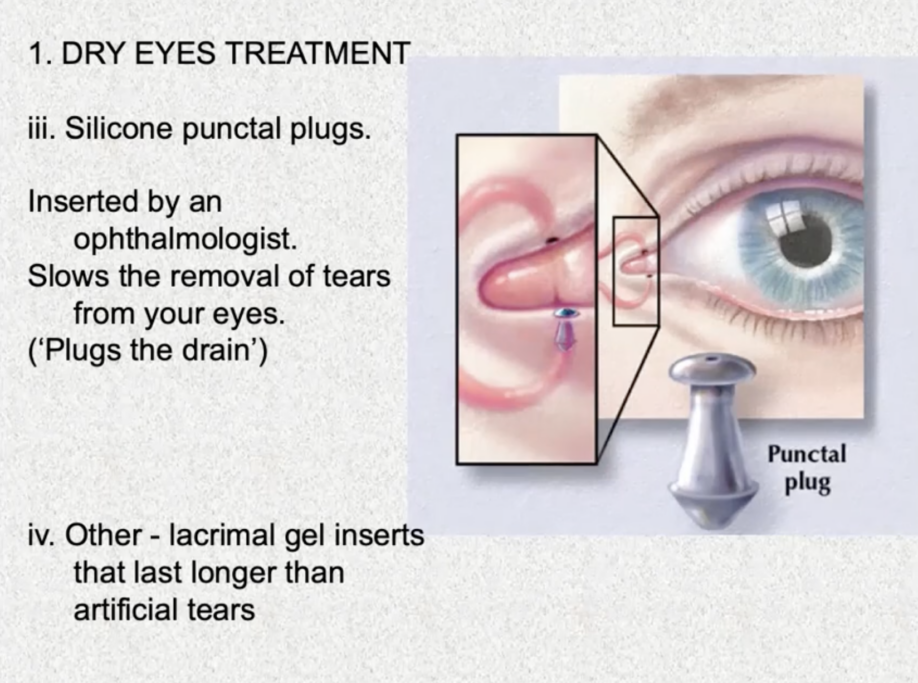
- Silicone punctal plugs
- Inserted by an opthalmologist
- Plugs the drain where tears are removed from your eye into your nose. This slows the removal of tears (natural or artificial) from your eyes, allowing your eyes to stay moist longer.
- Other – lacrimal gel inserts that last longer than artificial tears
- Inserted by an ophthalmologist
2. Blepharitis
Cause: Inflammation of the eyelids
- Meibomian glands in the lower edge of the eyelids – secrete oily film to help lubricate the eye and prevent evaporation of watery tear film.
- Related to increased sebum production and seborrheic dermatitis, which could be a manifestation of autonomic dysfunction in Parkinson’s disease. Meibomitis is like having seborrheic dermatitis of the eyelid.
- Can cause or aggravate dry eyes because the meibomian glands get blocked, reducing tear production.
Symptoms:
- Red eyes, red swollen lids
- Gritty, burning sensation (due to dry eye)
- Excessive tearing (due to dry eye)
- Itchy lids
- Crusting or matting of eyelashes in the morning
- Flaking or scaling of the eyelid skin
- Light sensitivity
- Blurred vision
Treatment: (in order of progression)
- Longstanding commitment to lid hygiene:
- morning warm compresses on lids for 5-10 minutes daily, up to 4 times daily during flare-ups
- massage the eyelids
- wipe lid margins with baby shampoo/water with a Q-tip or cloth
- Topical antibiotics (erythromycin) or systemic antibiotics (tetracycline) for bad cases
- Topical steroids for acute flares
- cyclosporine (immunosuppressant) eye drops ‘Restasis’
B. Vision in Parkinson’s Disease
1. Retina
Amacrine cells in the retina use dopamine as a neurotransmitter. Loss of dopamine function here could reduce:
- acuity (sharpness of central vision)
- color vision
- contrast sensitivity (ability to see fine shades of grey/shadow) – just as important as acuity
Dr. Barton doesn’t find a lot of people with PD complaining of these issues.
“Optical coherence tomography” – a simple non-invasive way to measure the thickness of the retina. If there are dopamine cells in the retina, can this show loss of retinal thickness in PD or other parkinsonism disorders, like progressive supranuclar palsy (PSP)?
Dr. Barton’s research team looked at this in 2020 and found that the retinal nerve fiber layer is reduced in those with PSP but not in those with PD.
Researchers don’t yet have a good way of measuring the inner nuclear layer (where dopaminergic amacrine cells live statistically), just the outer nerve layer. The inner layer is thinner and more subtle, but Dr. Barton believes they will figure it out.
2. Brain / Visual Cortex
Problems reported in identifying faces, facial expressions, spatial navigation
These all require a lot of brain network involvement
Not really a cause of major symptoms…or so we think…
Diffuse Lewy Body disease (DLB) – sometimes the degeneration is more widespread than just the substantia nigra. DLB includes both Parkinson disease dementia (PDD) and Lewy Body dementia (LBD). Because more of the brain is affected by Lewy Bodies, these patients have more cognitive issues, including dementia, than those with PD.
3. Hallucinations
up to 25% of patients with Parkinson’s disease
Exclusively visual, and complex (i.e., figures, faces, objects)
- Not like schizophrenia, which are usually auditory
- Not vague, but concrete. Often animals, children, etc.
Risk factors:
- duration and severity of Parkinson’s (the longer you’ve had PD, the more likely you are to have dementia and/or hallucinations)
- depression
- insomnia (may cause more confusion)
- cognitive impairment (early dementia)
Cause:
Could be related to disruption of REM sleep. REM Sleep Behavior Disorder (RBD) is often a prodromal symptom of PD and DLB.
Hallucinations can also occur as a side effect of L-dopa and dopaminergic drugs. Medication adjustment may resolve hallucinations, entirely.
May be Diffuse Lewy Body disease (DLB), rather than PD. People with DLB have:
- parkinsonism (PD-like motor problems)
- sleep-wake cycle inversion (tend to nap during the day and up at night)
- periodic confusion (fluctuating cognition)
- hallucinations in 90%
Hallucinations may correlate with having Lewy bodies in the anterior temporal lobe.
May be disruption of projections between midbrain and pons in the brainstem may impair REM sleep control. This would explain inverted sleep-wake cycle and hallucinations.
Treatment:
- remove or lower the dose of drugs that increase risk of hallucinations
- improve correctible problems with vision
- We know people with ‘visual deprivation’ (due to cataracts, stroke, etc.) may have release hallucinations. Seems like, in the absence of visual input, the brain starts to ‘make stuff up.’
- update eyeglass prescription
- remove cataracts
- corneal replacement
- drugs for Alzheimer’s (rivastigmine/Exelon) or REM sleep disorders (clonazepam/Klonopin)
C. Eye Movements in Parkinsonism
1. Convergence insufficiency
Most common cause of complaints of double vision in Parkinson’s: 30-50% of patients have this to some degree, but it doesn’t bother everybody.
Occasionally, Dr. Barton will tell someone with PD they have convergence insufficiency and the patient will not have noticed. Dr. Barton said it is possible in these cases the brain is suppressing the image from the second eye, or they are able to converge the images with concentration.
Symptoms:
- horizontal double vision (images are side-by-side)
- blurred vision, especially if the unconverged images are not far apart
- ocular ‘fatigue’/strain
Convergence is turning your eyes inward to look at something close, like reading or watching TV. With convergence insufficiency your eyes can’t align, and you see double.
Because your eyes are facing relatively straight forward, convergence is not required when looking at objects in the distance.
Cause:
Neurons that control convergence are located in the midbrain.
Convergence insufficiency may correlate with severity of PD.
People with parkinsonism disorders can have convergence insufficiency, too.
Treatment:
- Convergence exercises?
- Pencil push ups – look at a pencil as you move it closer to your eyes
- Known to work in kids, but effectiveness is unknown in adults
- Due to the neurodegenerative nature of PD & parkinsonism disorders, convergence and other eye issues will continue to get worse. So, if helpful, the effect will be temporary.
Adaptive strategies:
- Patch one eye when reading
- Put prisms in reading glasses
- Downsides
- need to get the size of the prism exactly right
- may change with time
- plastic stick-on prisms are less costly than replacing lenses
2. Square wave jerks
Small rapid eye movements that take the eye away from what you are trying to fixate on, then back again.
To have some is NORMAL. If you have too many, doctors wonder if there is a health problem.
Especially large wave in progressive nuclear palsy (PSP)
Not really noticeable to the patient, but the more frequent the square wave jerks, the slower you read
[short video of an eye experiencing square wave jerk.]
Cause:
Nothing is really known.
Treatment:
Anecdotal evidence that deep brain stimulation of the subthalamic nuclei might help
Adaptive strategy – read bigger text so slight jerk doesn’t take your eye off the text entirely
3. Vertical Gaze Palsy
Vertical gaze is the ability to look up and down. A key clue that you have PSP, rather than PD, is difficulty in looking up or down.
If you have:
- early falls
- little, if any, tremor
- stiff neck and back
- minimal improvement with L-dopa treatment
…you will probably be sent for a gaze assessment by a neuro-ophthalmologist
Problems caused by difficulty looking down:
- reading – we tend to read with books or ipads in our lap
- If you have no problem reading on a computer, it may be because you are not looking down at it.
- going down stairs
- eating meals – ‘dirty shirt’ sign because they tend to spill
All of this is compounded if you also have a stiff neck and can’t tip your head down, either.
Treatment:
Adaptive strategies
- prisms in glasses – bend the light so you don’t have to look down so far
- book holder on a table or music stand
- bring plate closer to mouth
4. Ocular dyskinesia
- During ‘ON phase’ with Sinemet, patients can have limb dyskinesia (excessive involuntary movements). Most people have seen Michael J. Fox with dyskinesia.
- 10-15% of the time there are similar dyskinetic movement of the eyes
- Usually not symptomatic
- Turning on a subthalamic stimulator can sometimes cause the eyes to deviate to the other side. Not something you want to do.
[Short video showing ocular dyskinesia]
Treatment:
As with limb dyskinesias, medication adjustment to smooth out peak ‘ON’ medication periods may help.
5. Can Eye Movements Help in Diagnosis?
What do you mean by, “diagnosis?”
First, detect if someone has PD, or not.
- Studies that have looked at this are comparing people with PD to healthy controls.
- In clinical practice, patients come to the neurologist because something’s wrong. The neurologist’s job it to figure out which of several possible disease.
There have been several studies looking at this question recently. Dr. Barton selected two to share.
- The first showed certain kinds of eye movements are affected, but not all. People with PD didn’t have difficulty tracking moving targets. People with PD, brain jury, depression, and schizophrenia have more difficulty than healthy controls glancing away from a stimulus when prompted (antisaccade errors).
- The second showed the combination of too many square wave jerks, delayed saccades, too-short upward saccades, and trouble following a moving target will identify 78% of those with PD.
Dr. Barton also shared a study which detected if someone has PD by measuring pervasive (micro) ocular tremor over time.
- Ocular tremor has been picked up by the company, RightEye, LLC, which offers testing and therapies for those with PD, autism, etc.
- Dr. Barton is concerned about this company’s claims because:
- The last scientific article from this group was published in 2014.
- They claim thousands have been tested with 100% accuracy, but where’s the data?
- They’re marketing to physicians selling the test kit promises up to $200K annual increased revenue. This is not patient-focused, but a clear conflict of interest.
BUT…
The studies compare their results against the neurologist’s diagnosis as the ‘gold standard’ – there is no other standard of diagnosis in these papers (e.g. autopsy)
So…eye movement tests can’t be shown to be better than the neurologist. If they had autopsy results showing whether the neurologist got the diagnosis right and if the eye movement test got the diagnosis right, that would be determinant of the effectiveness of the eye movement tests.
What would be better is a study of patients at an early stage, when we don’t know the diagnosis, and follow up to see who gets PD later…
…and see which is more accurate at predicting the future, the eye movements or the neurologist’s exam…
Maybe someone is doing this, but Dr. Barton hasn’t seen it, yet.
Second, determine if they have PD or some other form of parkinsonism.
This is when Dr. Barton is asked to help in the diagnostic process, to distinguish between:
- diffuse Lewy body disease (DLB) – hallucinations
- multi system atrophy (MSA), type C (cerebellum) – gaze-evoked nystagmus (large fixation instability)
- progressive supranuclear palsy (PSP) – vertical gaze palsy
These are much rarer conditions, hence less data on when these eye movement abnormalities become useful in distinguishing diagnosis.
Finally, determine if they have some ‘complication’ of PD (e.g., dementia), a diffuse Lewy body disorder (DLB).
Dr. Barton shared a study that showed stability of fixation tended to correlate with cognitive measures on testing.
The gold standard for cognitive decline is neuropsychological testing, so one cannot prove that the eye movements are better than neuropsychological tests in detecting cognitive problems.
At best you can show eye movements are as good as neuropsychological testing, although eye movement tests may be easier to administer. Neuropsychological testing is a half day with a neuropsychologist testing memory, attention, visual-spatial perception, etc., whereas eye movement tests take 10 minutes.
Question & Answers
Question. Can cataract surgery play into any of this?
Answer. There is a potential role that having very bad vision may predispose you to having release hallucinations. It might be that having mildly bad vision in combination with PD may also predispose you to having hallucinations.
Dr. Barton can’t say there’s a study that shows there is a 50% or 75% reduction in hallucinations among those who have had cataract surgery, but it is something people have speculated about.
Question. Please talk about retinal detachment.
Answer. This is not specific to PD, but not something you want to have happen.
When someone has retinal detachment, they are unable to see in the area that is no longer attached. If the detached area is the macula, that is really bad because the macula is the single most useful area of your vision, straight ahead of you. You use your macula to read. You can’t read with your side vision.
There are ways to reattach the retina and improve your vision if you get this attended too quickly. If you don’t attend to retinal detachment, the hole in your vision may get bigger.
You would know you have retinal detachment if there is an area in which you can’t see. You may also have a sudden shower of flashes and floaters.
Dr. Barton doesn’t repair retinal detachments, but he has treated patients with retinal detachment repairs. The repairs seem to work quite well for many years.
Question. A listener asked about depth perception with regard to a tile pattern on the floor.
Answer. Depth perception is not so well studied. This could be related to face, object, and visual-spatial recognition.
There are ways to measure depth perception in the clinic with stereopsis. This is like looking at 3-D movies. To determine if depth perception is why you’re having trouble with the tile pattern on your floor, go to a 3-D movie and see if you can see the 3-D effect. If you can, maybe there is something else going on with your tiles.
Question. Please comment on plastic stick-on prisms.
Answer. A frensel prism is a plastic stick-on prism. They only cost about $40 (in Canada). We use them to let a person try a prism without committing to a glass prism. This also helps determine the right size prism to make in glass if the patient likes using prism glasses.
Every optometrist has a bunch. They will cut out the size most likely to be helpful to you and stick it on your glasses with some water. You can take it off to clean it. It is not as clear as glass, but enough to tell whether prisms are right for you.
Question. Is there a link to how to do convergence exercises?
Answer. Not that Dr. Barton knows, but your optometrist may be able to teach them to you.
Remember, evidence is only on the effectiveness in children so Dr. Barton is reluctant to recommend them for those with neurodegenerative disorders.
Also, the in-office exercises are shown to be more effective than doing them at home, but that comes at a cost. Each in office therapy sessions is $160 CAD, and they recommend you do 6-10 sessions.
The exercises are generally moving an object from far to near and following it with your eyes. It can be something on a string.
A therapist may have a screen version where the patient wears polarized glasses, so one eye sees one thing and the other eye sees another image. The therapist can make those images move closer or farther. This simulates an object moving closer or farther away.
At home you can use the eraser on the end of a pencil. As the pencil is moving toward you, where the image starts to break into two, hold the pencil there and try to merge a single image with some effort. As you repeat the exercise, it may get easier, and you may be able to bring the pencil closer and maintain a single image.
Question. A listener asks if they should have a neuro-ophthalmologist on their care team?
Answer. Not if you think you have dry eyes or blepharitis. Your optometrist can manage those issues very well.
If you have double vision, see a general ophthalmologist. They can either help you or refer you to the right kind of specialist, if necessary.
For example, if you have double vision and when you close one eye you still have double vision, that is not because your eyes are misaligned. That is because the light getting into one eye is being bent or distorted a bit. It can be because of dry eye or a cataract.
Question. Can bifocals cause the same kind of up/down eye movement problems?
Answer. No, but they can be a problem for people with up/down eye movement problems. Bifocals and progressive lenses are set up so that when you want to look close, you look through the bottom part of the glass. If you have trouble looking down, you can’t move your eyes downward to take advantage of the bifocal part of the lens.
People with up/down eye movement problems are better off getting separate distance and reader glasses so the whole lens is the same prescription, and you can see well regardless of where your eye is focused.
Question. A listener asked about preservatives in eye drops.
Answer. There are preservative-free eye drops in single-use tubes. Dr. Barton feels this is a terrible waste of plastic but if your eyes are irritated by drops with preservatives, use them!
He is not bothered by the preservatives and is not worried about getting exposed to anything weird. When he needs eye drops, he uses the larger bottle with preservatives in them. In fact, he feels if eye drops will be sitting around on the shelf for a long time, preservatives will keep things from growing in the bottle.
Question. A listener’s husband has trouble keeping his eyes open. His eyes close and he cannot open them frequently.
Answer. Eye lids can be abnormal. The most common problem with PD and parkinsonism is reduced blinking. But there are some people who have blepharospasm. It is an involuntary eye movement. It is a focal dystonia of the eyelid so that they squeeze shut and you have trouble opening your eyes. It is a problem with the muscles of the eyelid, not the muscles around the eye socket.
The best treatment is botulinum toxin (Botox). It weakens the muscle marginally so you can open your eyes when you want to. In the old days oral medications were tried to treat this but they are ineffective.
Some people keep their eyes closed because their eyes hurt. This can be due to dry eye, light sensitivity, etc. Treatment for this is not botulinum toxin, but treatment for the underlying problem making the eyes hurt.
Question. What type of muscle controls eye movements?
Answer. Each eye has six small muscles that move the eyes in every direction. They differ a bit from limb muscles, having a higher mitochondria content. You make an eye movement three times every second you are awake. These are highly active muscles.
Their small size or difference from limb or smooth muscles doesn’t make them more vulnerable to Parkinson’s because PD is not about the muscles. Some muscle diseases do affect eye muscles more, but PD is about central control in the brain.
It so happens that the structures that control vertical gaze and convergence are in the midbrain close to the structures affected by PD. The structures that control looking sideways are lower down in the pons, so those are unaffected by PD and parkinsonism.
Question. Does dopamine affect acuity, color vision, and contrast?
Answer. Dr. Barton doesn’t know.
Question. Simon has too much tears. They overflow his eyes. Is this common in PD? Simon has had PD for six years.
Answer. When you have dry eyes the surface of your eye gets irritated. You may or may not feel that irritation. You cannot use the feeling of irritation as a reliable guide as to whether your cornea is drying out.
If your cornea dries out, one thing your brain will do when it senses that drying is a reflexive tearing. This is just like getting something in your eye, your eyes tear as a reflexive defense against pain and damage.
This is the most common reason tears overflow. Not because the primary problem is that you are making too many tears, but that your cornea is dry, and your body is making tears to compensate. The solution is to make your cornea more comfortable using dry eye treatments.
Question. Please talk about blue lens glasses when watching TV.
Answer. If you are a bit light sensitive the first thing is to make sure you don’t have blepharitis or dry eye. Because the treatment for that is lid hygiene, not worrying about lenses.
You can have photosensitivity for other reasons besides PD. Dr. Barton sees a lot of people with traumatic brain injury complain of photosensitivity. We don’t understand why.
The evidence that some types of lenses are better than others is fuzzy. People recommend blue blockers because they believe those affect the kind of light those neurons absorb more. Studies Dr. Barton has seen with respect to traumatic brain injury don’t show blue blocker are the right kind of lens for everybody. The kind of lens people choose after the studies is all over the place.
Ask your optometrist if you can try several kinds of filters to see which works best for you while watching TV. You can also try turning down the contrast on your TV set.
Question. A listener asked about drinking enough fluids to treat dry eye.
Answer. That might help, but if you have blepharitis, it may not be enough to resolve the situation.
There may be other contributing factors, like wind in your face. This is when Dr. Barton gets dry eyes, riding his bike for hours.
Some people notice their C-PAP machine tends to blow air. If your mask doesn’t fit properly, it may blow up your face night after night and contribute to dry eyes.
Question. Andrea developed vision problems 5-6 years after her PD diagnosis. She is skeptical eye tests would have provided early detection in her case.
Answer. Dr. Barton agrees. All the studies on people who have been diagnosed for a number of years tell you there is something abnormal about the way the eyes move but won’t tell you whether it’s helpful when you study somebody early on.
These studies are hard because you have to follow people for a few years to see what the answer is.
Question. What is the eyelid regimen for crusty eyelids.
Answer. Get a washcloth wet with warm water (not too hot). Place that cloth over your eyes and keep it there for 5-10 minutes. Then, rub the cloth across your eyelids to gently remove the crustiness.
Some people find putting a little degreasing baby shampoo on the washcloth might be more effective at removing the crustiness.
Question. Is optic nerve palsy a symptom of Parkinson’s?
Answer. Optic neuropathy is not a palsy.
The optic nerve is responsible for seeing vision and bringing vision information from your retina to your brain. Optic neuropathy is the failure of transmitting light from your retina to your brain, either in part or in whole.
A palsy is a weakness. You can have ocular motor palsy in which the muscles responsible for moving the eye around don’t work and you see double vision because of that.
Neither are PD problems.
Question. With looking down, what lens do you recommend?
Answer. A progressive lens is like a bifocal and changes refraction so you can focus up close and far.
Usually, when people put a prism on a lens, they only put one prism. Although they can put a partial prism where they just put the prism over the bottom part of your lens. This is where you would use a plastic prism.
Question. Steven experiences a vertical stacking of images, particular in the distance, which diminishes as he gets closer to the object. This also be eliminated by covering or closing either eye. What’s causing this? Is it Parkinson’s related? It started about a year prior to his PD diagnosis.
Answer. Vertical double image in just one eye can be a cataract or retinal problem. That is not the case for Steven.
Try to figure out how it changes depending on where you look. Steven has done the near/far thing, now he should see if the double vision changes when he looks up, down, left, or right. That can help determine if the problem is with a muscle or fits a pattern to make a diagnosis.
It could be fourth nerve palsy or other issue. Some people are born with a fourth nerve palsy they don’t even know about until they age or have something like PD.
It is not uncommon to have vertical double vision in PD, but vertical double vision may not have anything to do with PD. There is some sort of ocular misalignment going on. Since it has been going on for years, it is not something terribly serious. Steven should have an assessment.
Question. Is it common for someone with PD and 20/20 vision to have blurred vision and have difficulty reading a newspaper.
Answer. Check to make sure you have 20/20 vision up close with appropriate vision correction. Even then you may have a convergence problem. Go see your optometrist!